Problem 33 Cough, dyspnoea and fever in a 55-year-old man
A 55-year-old man presents with 3 days of anorexia, headache, general weakness, aches and pains all over his body. He thought he had the flu and has been treating himself with paracetamol.
However, in the last 24 hours he has become very unwell, with a high fever, irritating dry cough, breathlessness and diarrhoea and he has vomited a number of times. He has no pleuritic pain but has a dull generalized ache in his abdomen. There is no significant past medical history. He has no pets, animal contacts or recent holiday travel but likes gardening. He smokes about 20 cigarettes a day and consumes 30–50 g of alcohol daily. He is not on any regular medications and has no known allergies.
On examination he looks unwell and flushed. He is orientated but agitated and easily distracted. He has a temperature of 39.5°C. The patient is not cyanosed, clubbed, jaundiced or anaemic. He has dry mucous membranes and a coated tongue. His pulse rate is 105 bpm and regular, his blood pressure is 120/75 mmHg and his oxygen–haemoglobin saturation is 90%. His cardiovascular system is otherwise normal. His respiratory rate is 30 breaths per minute and he has a hacking cough productive of small amounts of mucoid sputum. His chest is resonant and the breath sounds vesicular. There are scattered inspiratory crepitations throughout the right lung only. His abdomen is soft and non-tender. There is no neck stiffness and there are no focal neurological signs.
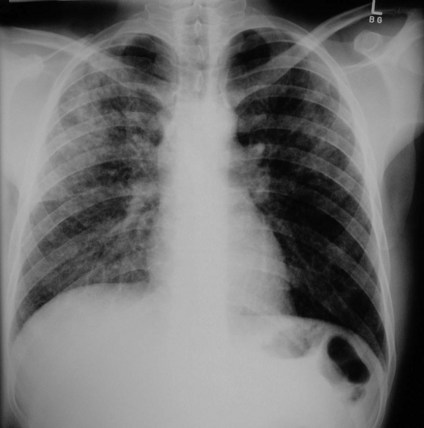
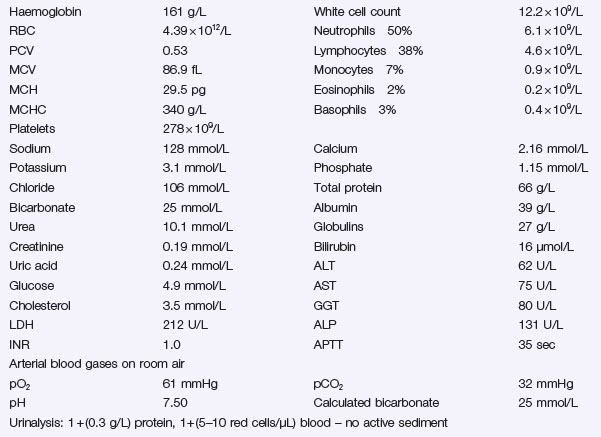
You review the chest X-ray Figure 33.1 and the results of your other tests can be seen in Investigation 33.1.