Chapter 12 Cough, Cold, and Allergy
Antitussives




Moa (Mechanism of Action)
 Antitussives are cough suppressants. There are two ways to inhibit coughing: centrally and peripherally.
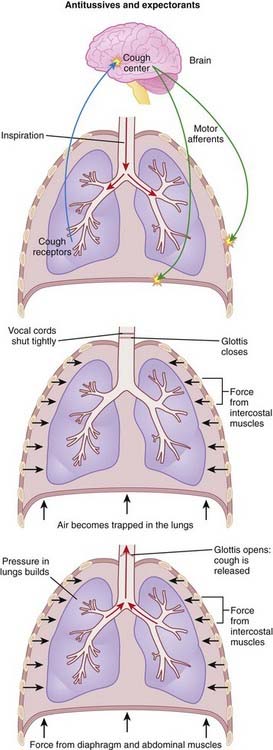
Antitussives are cough suppressants. There are two ways to inhibit coughing: centrally and peripherally. Cough is normally produced through the stimulation of sensory receptors of the glossopharyngeal and vagus nerves, innervating the mucous membranes of the lower pharynx, larynx, trachea, and smaller airways of the respiratory system. The receptors then transmit the signal to the cough center in the brain, which then triggers a reflex motor response that results in contraction of the muscles to close the glottis (vocal cords) and contraction of the muscles of expiration. The result is a sudden increase in intrathoracic pressure, followed by relaxation of the vocal cords, resulting in rapid expulsion of air (Figure 12-1).
Cough is normally produced through the stimulation of sensory receptors of the glossopharyngeal and vagus nerves, innervating the mucous membranes of the lower pharynx, larynx, trachea, and smaller airways of the respiratory system. The receptors then transmit the signal to the cough center in the brain, which then triggers a reflex motor response that results in contraction of the muscles to close the glottis (vocal cords) and contraction of the muscles of expiration. The result is a sudden increase in intrathoracic pressure, followed by relaxation of the vocal cords, resulting in rapid expulsion of air (Figure 12-1).









Important Notes
 Dextromethorphan was developed in an attempt to create a cough suppressant with the efficacy of codeine but with none of the central nervous system (CNS) side effects such as euphoria. Dextromethorphan therefore has little or no ability to induce euphoria and therefore is available without a prescription and without pharmacist consultation in most jurisdictions.
Dextromethorphan was developed in an attempt to create a cough suppressant with the efficacy of codeine but with none of the central nervous system (CNS) side effects such as euphoria. Dextromethorphan therefore has little or no ability to induce euphoria and therefore is available without a prescription and without pharmacist consultation in most jurisdictions.







Evidence
Over-the-Counter Preparations for Acute Cough
 A 2008 Cochrane review (25 trials, N = 3492 participants) assessed the effects of over-the-counter (OTC) cough preparations for acute cough. Six trials in adults had variable results for antitussives versus placebo. Of the two trials involving expectorants, one showed benefit versus placebo whereas the other did not. In children, antitussives (two trials), antihistamines (two trials), antihistamine-decongestant combinations (two trials), and antitussive-bronchodilator combinations were no more effective than placebo. No trials were found of expectorants, but one trial showed benefit of a mucolytic versus placebo.
A 2008 Cochrane review (25 trials, N = 3492 participants) assessed the effects of over-the-counter (OTC) cough preparations for acute cough. Six trials in adults had variable results for antitussives versus placebo. Of the two trials involving expectorants, one showed benefit versus placebo whereas the other did not. In children, antitussives (two trials), antihistamines (two trials), antihistamine-decongestant combinations (two trials), and antitussive-bronchodilator combinations were no more effective than placebo. No trials were found of expectorants, but one trial showed benefit of a mucolytic versus placebo.

Expectorants


Moa (Mechanism of Action)
 Mucus serves as an airway lubricant and functions as a first level of immune defense. When mucus becomes thickened and/or dried out by infections, the functions of the mucus, including the clearing of infections, becomes impaired.
Mucus serves as an airway lubricant and functions as a first level of immune defense. When mucus becomes thickened and/or dried out by infections, the functions of the mucus, including the clearing of infections, becomes impaired.








Important Notes
 There has been a longstanding controversy over the use of expectorants. This is partly because of the limited data demonstrating their efficacy.
There has been a longstanding controversy over the use of expectorants. This is partly because of the limited data demonstrating their efficacy.

Evidence
Over-the-Counter Preparations for Acute Cough
 A 2008 Cochrane review (25 trials, N = 3492 participants) assessed the effects of OTC cough preparations for acute cough. Of the two trials involving expectorants, one showed benefit versus placebo whereas the other did not. In children, no trials were found of expectorants, but one trial showed benefit of a mucolytic versus placebo.
A 2008 Cochrane review (25 trials, N = 3492 participants) assessed the effects of OTC cough preparations for acute cough. Of the two trials involving expectorants, one showed benefit versus placebo whereas the other did not. In children, no trials were found of expectorants, but one trial showed benefit of a mucolytic versus placebo.



