31 Constrictive pericarditis
Salient features
Examination
• The patient may appear cachectic.
• Pulse may be regular or irregularly irregular (one-third have atrial fibrillation).
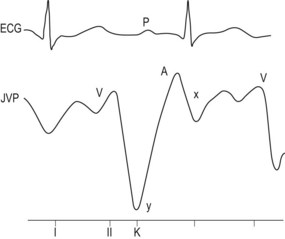
• Prominent ‘x’ and ‘y’ descents in the JVP and the level of the jugular venous pulse may rise with inspiration (Kussmaul’s sign; Fig. 31.1).
• Apex beat is not palpable and there may be apical systolic retraction (Broadbent sign).
• Early diastolic pericardial knock along the left sternal border, which may be accentuated by inspiration.
• Lungs are clear but there may be pleural effusion.
• Markedly distended abdomen with hepatomegaly and ascites.