Chapter 14 Constipation and diarrhoea
Constipation
Diarrhoea
Constipation
In Western populations, 90% of people defaecate between three times a day and once every 3 days. It is clear, therefore, that to base a definition of constipation on frequency alone is problematic. What is perceived to be constipation by one individual may be normal to another. Most definitions of constipation include infrequent bowel action of twice a week or less that involves straining to pass hard faeces and which may be accompanied by a sensation of pain or incomplete evacuation. A pragmatic definition would simply be the passage of hard stools less frequently than the patient’s own normal pattern. Standard criteria for the diagnosis of diarrhoea are available (Longstreth et al., 2006), although they are seldom used in practice.
Aetiology
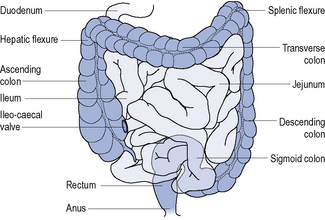
The digestive system can be divided into the upper and lower gastro-intestinal tract. The upper gastro-intestinal tract starts at the mouth and includes the oesophagus and stomach and isresponsible for the ingestion and digestion of food. The lower gastro-intestinal tract consists of the small intestine, large intestine (colon), rectum and anus (Fig. 14.1) and is responsible for the absorption of nutrients, conserving body water and electrolytes, drying the faeces and elimination.
Differential diagnosis
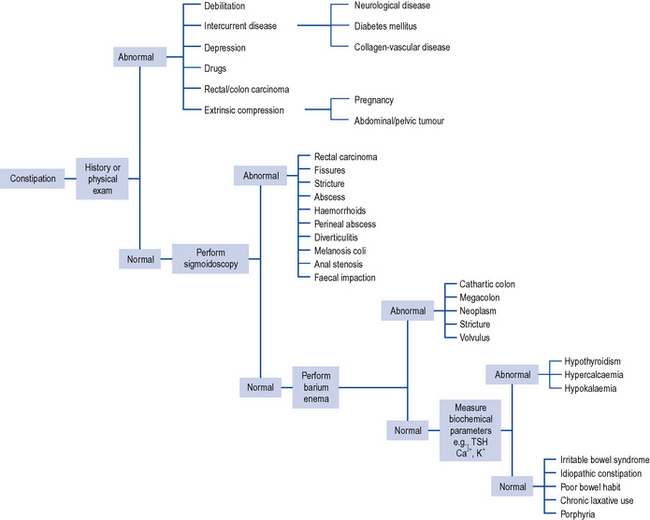
Constipation is a symptom and not a disease and can be caused by many different factors (Table 14.1) but the overwhelming majority of cases in non-elderly patients will be due to lack of dietary fibre. To aid diagnosis, questions need to be asked about the frequency and consistency of stools, nausea, vomiting, abdominal pain, distension, discomfort, mobility, diet and other concurrent symptoms or disorders the patient may be experiencing. It may also be necessary to ask about access to a toilet or commode. The individual with limited mobility may suppress the urge to defaecate because of difficulty in getting to the toilet. Likewise, lack of privacy or dependency on a nurse or carer for toileting may result in urge suppression that precipitates constipation or exacerbates an underlying predisposition. Patients with unexplained constipation of recent onset or a sudden aggravation of existing constipation associated with abdominal pain and the passage of blood or mucus, and long-standing constipation unresponsive to treatment require further investigation. Investigations include sigmoidoscopy/colonoscopy, barium enema, full blood count and biochemical monitoring including thyroid function tests (Fig. 14.2).
Table 14.1 Causes of constipation
| Cause | Comment |
|---|---|
| Poor diet | Diets high in animal fats, for example, meats, dairy products, eggs, and refined sugar, for example, sweets, but low in fibre predispose to constipation |
| Irritable bowel syndrome | Spasm of colon delays transit of intestinal contents. Patients have a history of alternating constipation and diarrhoea |
| Poor bowel habit | Ignoring and suppressing the urge to have a bowel movement will contribute to constipation |
| Laxative abuse | Habitual consumption of laxatives necessitates increase in dose over time until intestine becomes atonic and unable to function without laxative stimulation |
| Travel | Changes in lifestyle, daily routine, diet and drinking water may all contribute to constipation |
| Hormone disturbances | For example, hypothyroidism, diabetes. Other clinical signs should be more prominent, for example, lethargy and cold intolerance in hypothyroidism and increased urination and thirst in diabetes |
| Pregnancy | Mechanical pressure of womb on intestine and hormonal changes, for example, high levels of progesterone |
| Fissures and haemorrhoids | Painful disorders of the anus often lead patients to suppress defaecation, leading to constipation |
| Diseases | Many disease states may have constipation as a symptom, for example, scleroderma, lupus, multiple sclerosis, depression, Parkinson’s disease, stroke |
| Mechanical compression | Scarring, inflammation around diverticula and tumours can produce mechanical compression of intestine |
| Nerve damage | Spinal cord injuries and tumours pressing on the spinal cord affect nerves that lead to intestine |
| Colonic motility disorders | Peristaltic activity of intestine may be ineffective, resulting in colonic inertia |
| Medication | See Table 14.2 |
| Dehydration | Insufficient fluid intake or excessive fluid loss. Water and other fluids add bulk to stools, making bowel movements soft and easier to pass |
| Immobility | Prolonged bedrest after an accident, during an illness or general lack of exercise |
| Electrolyte abnormalities | Hypercalcaemia, hypokalaemia |
General management
If the patient is taking medication for a concurrent disorder this must be assessed for its propensity to cause constipation. In the UK, over 700 medicinal products, including ophthalmic preparations, have constipation listed as a possible side effect. Common examples of medicines involved are presented in Table 14.2.
Table 14.2 Examples of medicines known to cause constipation (frequency defined as very common [>10%] or common [1–10%])
| α-Blocker | Prazosin |
| Antacid | Aluminium and calcium salts |
| Anticholinergic | Trihexyphenidyl, hyoscine, oxybutynin, procyclidine, tolterodine |
| Antidepressant | Tricyclics, SSRIs, reboxetine, venlafaxine, duloxetine, mirtazepine |
| Antiemetic | Palonosetron, dolasetron, aprepitant |
| Antiepileptic | Carbamazepine, oxcarbazepine |
| Antipsychotic | Phenothiazines, haloperidol, pimozide and atypical antipsychotics such as amisulpride, aripiprazole, olanzapine, quetiapine, risperidone, zotepine, clozapine |
| Antiviral | Foscarnet |
| β-Blocker | Oxprenolol, bisoprolol, nebivolol; other β-blockers cause constipation more rarely |
| Bisphosphonate | Alendronic acid |
| CNS stimulant | Atomoxetine |
| Calcium channel blocker | Diltiazem, verapamil |
| Cytotoxic | Bortezomib, buserelin, cladribine, docetaxel, doxorubicin, exemestane, gemcitabine, irinotecan, mitozantrone, pentostatin, temozolomide, topotecan, vinblastine, vincristine, vindesine, vinorelbine |
| Dopaminergic | Amantadine, bromocriptine, carbegolide, entacapone, tolcapone, levodopa, pergolide, pramipexole, quinagolide |
| Growth hormone antagonist | Pegvisomant |
| Immunosuppressant | Basiliximab, mycophenolate, tacrolimus |
| Lipid-lowering agent | Colestyramine, colestipol, rosuvastatin, atorvastatin (other statins uncommon) gemfibrozil |
| Iron | Ferrous sulphate |
| Metabolic disorder | Miglustat |
| Muscle relaxant | Baclofen |
| NSAID | Meloxicam; other NSAIDs, for example, aceclofenac, and COX-2 inhibitors reported as uncommon |
| Smoking cessation | Bupropion |
| Opioid analgesic | All opioid analgesics and derivatives |
| Ulcer healing | All proton pump inhibitors, sucralfate |
Non-drug treatment
Non-drug treatment is advocated as first-line therapy for all patient groups, except those who are terminally ill. This often includes advising an increase in fluid intake at the same time as reducing strong or excessive intake of tea or coffee, since these act as a diuretic and serve to make constipation worse.It is generally recommended that fibre intake in the form of fruit, vegetables, cereals, grain foods, wholemeal bread, etc. be increased to about 30 g/day. The amounts of fibre in commonly eaten foods have been published (MeReC, 2004). Such a diet should be tried for at least 1 month to determine if it has an effect. Most will notice an effect within 3–5 days. Unfortunately, a high-fibre diet is not without problems, with patients complaining of flatulence, bloating and distension, although these effects should diminish over a period of several months. Patients who increase their fibre intake must also be advised to drink 2 L of water a day. Where an intake of this volume cannot be ingested it will be necessary to avoid increasing dietary fibre. An increased level of exercise should also accompany the raised fibre intake as this is thought to help relax and contract the abdominal muscles and help food move more efficiently through the gut.
Drug treatment
Drug treatment is indicated where there is faecal impaction, constipation associated with illness, surgery, pregnancy, poor diet, where the constipation is drug induced, where bowel strain is undesirable, and as part of bowel preparation for surgery. The various laxatives available can be classified as bulk forming, stimulant, osmotic and faecal softeners. A systematic review (Tramonte et al., 1997) identified 36 trials involving 1815 participants that met their inclusion criteria. Twenty of the trials compared laxative against placebo or regular diet, 13 of which demonstrated statistically significant increases in bowel movement. The remaining 16 trials compared different types of laxatives with each other. The review concluded that laxative use was superior to placebo but due to a lack of comparative data could not conclude which laxative group was most efficacious. Further, more recent reviews have found good evidence that macrogols are effective, as are ispaghula husk and bisacodyl, although data is still lacking on which laxative is best (Frizelle and Barclay, 2007).



