OVERVIEW
- Depression and anxiety are common in patients with medically unexplained symptoms (MUS); most patients have elements of both
- MUS are not the same as depression and anxiety, although MUS predispose to emotional disorder and emotional disorders predispose to MUS
- Many patients with MUS will play down their emotional symptoms for fear of being mislabelled
- Questionnaires such as the Patient Health Questionnaire (PHQ9) and Generalized Anxiety Disorder scale (GAD7) or Hospital Anxiety and Depression Scale (HADS) can help patients see that their emotions are typical of depression or anxiety
Introduction
In this chapter we outline a clinical approach to the detection and assessment of depressive and anxiety disorders. Treatment is covered separately in Chapters 15–17.
Epidemiology
Major depressive disorder, diagnosed using standard criteria (see Box 4.1) is common in the general population and in patients with MUS. Typical population-based studies suggest a prevalence of around 2% with a lifetime incidence of 6–9% for women and 3–5% for men. It occurs across all ages with a peak incidence at around 40 years old.
Generalised anxiety disorder (Box 4.2) has a prevalence of 3-4% in woman and 2–3% in men. The prevalence of panic disorder (1%) (Box 4.3) and phobic disorders (1–2%) is slightly lower.
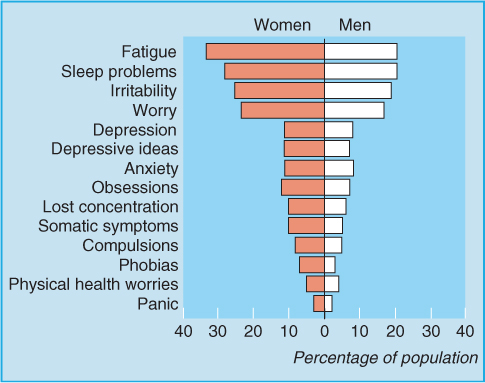
However, these psychiatric definitions of depressive and anxiety disorders were developed in secondary care where only a small proportion of those with symptoms of any of the emotional disorders are seen. At a population level the presence of symptoms of emotional disorder is continuously distributed (Figure 4.1) and the classical psychiatric diagnostic categories have limited value. In primary care most patients present with a mixed picture of anxiety and depression and meet the criteria for more than one diagnosis. Taken as a group depressive and anxiety disorders have a prevalence of around 10% in women and 5% in men.
Figure 4.1 Symptoms of depressive and anxiety disorders are continuously distributed in the population. Reprinted from Mayou R, Sharpe M, Carson A. (2003) ABC of Psychological Medicine. BMJ books, with permission from John Wiley & Sons Ltd.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


