Although communication can take many forms, the focus of this chapter is on verbal communication, which is composed of four constituent domains—speaking, listening, reading, and writing. Any or all of these four domains may variably be subject to age- and/or disease-related changes. The downstream effects of changes in the ability to communicate, regardless of the affected domain(s), are brought into sharp relief for people with life-limiting diseases. To better characterize communication at the end of life, this chapter addresses the nature of (1) age-related sensory and communication changes, (2) communication changes that result from terminal disease processes, (3) age-related and disease-related changes in cognition and their effect on communication, (4) the role of the speech-language pathologist (SLP) in providing services to people at the end of life, and (5) strategies for facilitation of communication at the end of life.
This chapter also addresses swallowing issues at the end of life, and the swallowing discussion is organized similarly to the section on communication. To better characterize swallowing at the end of life, the chapter addresses the nature of (1) age-related physiologic changes that can influence swallowing status, (2) changes in swallowing that result from terminal disease processes, (3) the influence of age-related and disease-related changes in cognition on swallowing, (4) the role of the SLP in providing dysphagia services to people at the end of life, and (5) strategies for facilitation of nutrition and hydration at the end of life.
As therapists, one of our goals is to work ourselves out of a job, in that we aim to discharge patients once therapy goals have been reached. Supporting communication at the end of life may seem antithetical to the ‘treat and discharge’ model of service provision, because at the end of life, improvement in function is not anticipated. Rather, as service providers, we aim to facilitate communication, in whatever form it may take—spoken, written, symbol-based, gestural, or some combination thereof—so that our patients can communicate with medical personnel, caregivers, family, and friends. Whereas functional abilities may be in decline at the end of life, communication remains one of the most important mainstays of end-of-life care. It is through this lens that preserving and/or ameliorating communication at the end of life is discussed.
20.2 Age-Related Sensory Changes
Research indicates that most people experience a variety of age-related sensory changes that can deleteriously influence the ability to communicate. The most common changes include a decrease in vision and/or hearing acuity.
Age-related vision changes may begin as early as the fourth decade of life; the most common vision change is presbyopia, which results from a loss of elasticity in the lens of the eye. This loss of elasticity decreases the eyes’ ability to accommodate to near stimuli. It also leads to decreased contrast sensitivity and delayed recovery from glare.
Other visual pathologies that can deleteriously influence vision status in older adults include cataracts, diabetic retinopathy, glaucoma, and age-related macular degeneration. Cataracts are a progressive retinal disorder causing blurred vision and impaired contrast sensitivity and can result in blindness if they are not addressed. Diabetic retinopathy can result in blurred, distorted vision in the central visual field and may result in retinal detachment. Glaucoma results from a malfunction of the eye’s drainage system and can cause the loss of the visual field. Age-related macular degeneration is the progressive loss of reading vision and sharp distance vision. Central vision is typically most affected, whereas peripheral vision is typically spared in this retinal disorder.
Changes in vision can have a number of effects on communication. Written communication—reading and/or writing—may be compromised secondary to visual disturbances. Difficulty with reading may interfere with the ability to use a communication display or device. Similarly, visual changes experienced by the frequent and familiar communication partners of people who already use some type of augmentative or alternative communication (AAC) display or device may interfere with established roles and routines in terms of communication. Adjustable font sizes and the ability to adjust or create visual contrast (e.g., heavy black print on a light background, increased background lighting, or better ambient lighting), on displays and/or devices may attenuate some of the visual difficulties that can interfere with communication.
If the visual disturbance is severe enough that it precludes access to written language, the patient may need to use other means of accessing print, such as having materials presented auditorily.
Age-related hearing changes include anatomical changes, such as narrowing of the external auditory canal, increased rigidity of the tympanic membrane, and ossicular atrophy 2; accumulation of cerumen, a reversible condition that results from excessive wax production; otosclerosis (immobilization of the stapes), which may be correctible with surgery; noise-induced hearing loss (typically irreversible); presbycusis 3; and changes in speech recognition. The changes in speech recognition are particularly important with respect to both the need for hearing aids and the accommodations necessary to either use or listen to a speech-generating device (SGD).
An issue of growing relevance for SLPs is that presbycusis may be accelerated and heightened by noise-induced hearing loss, 4 resulting in clinically more complex issues related to hearing loss in the aging population.
The combination of vision and hearing impairments results in dual sensory loss, which is increasingly common. 5, 6 In the context of this chapter, dual sensory loss pertains to individuals who became dually impaired in adulthood by the onset of age-related changes and/or age-related disease in sensory organs (e.g., presbycusis and macular degeneration). This dramatic change in sensory status for previously well individuals marks a serious shift in functional abilities. 7 Vision and audition provide the two major channels for language input via print, sound, and/or speech reading. Thus, dual sensory loss compounds communication impairment in complex ways, depending on the type of loss in each sensory system, the age at onset and nature of the onset of the loss, and the extent to which a person can cope with the losses. The SLP must further consider that dual sensory loss may occur in the context of multiple other comorbidities, both physical and psychological, that complicate the clinical management of the communication-related deficits.
Changes in tactile sensitivity and peripheral sensation often occur with age. 8, 9, 10 Peripheral nerve function that controls the sense of touch declines slightly with age. Two-point discrimination and vibratory sense both decrease with age. The ability to perceive painful stimuli is preserved in aging. However, aging may result in slowed reaction time for pulling away from painful stimuli.
Peripheral neuropathy is one of the most common neurologic disorders encountered in a general medical practice, with an estimated 2 to 7% of all patients having symptoms of neuropathy. 11 The Women’s Health and Aging Study indicated that 58% of women showed evidence of neuropathy by age 65. 12
Changes in hand function, such as a decrease in both grip strength and discriminative function, are also associated with aging 8 and may interfere with a person’s ability to use communication media, such as paper and pencil and all types of electronic devices (e.g., cell phones, electronic writing slates, mobile tablets, etc.). With the proliferation of mobile tablets and their reliance on touch interface, changes in tactile sensitivity and hand function may interfere with the use of these ubiquitous technologies. Changes in tactile sensitivity and hand function can diminish both the adoption and the adaptation to use of low- and/or high-technology AAC systems. Dimensions of AAC systems, such as weight, size, and method of interface, must be carefully considered in light of these changes.
Although not a sensory change, arthritis is a common condition in the aging population, and its prevalence and incidence are predicted to increase. 13 Arthritis causes swelling and inflammation of the joints and subsumes a range of illnesses and conditions, such as osteoarthritis (OA), rheumatoid arthritis (RA), and gout. When arthritis affects the hands, it can negatively influence written communication and/or use of an AAC system that requires direct selection. 14 To mitigate the effects of arthritis and its deleterious effect on swift and targeted movements of the hands, the SLP must consider whether a proposed AAC system supports modification of key size and sensitivity and duration of contact required with a key for selection, as well as screen/monitor size. Together, sensory and arthritic changes in hand function will influence the type of communication aids that may be used by an individual.
Age-associated changes in olfaction, such as a decline in the ability to identify odors, do not have a direct effect on communication and/or use of assistive devices but can be important diagnostically. Anosmia, the loss of the sense of smell, can be temporary or permanent, partial or complete. If any part of the olfactory pathway is damaged or destroyed, beginning with the nasal mucosa and ending with higher cortical areas where olfactory inputs are interpreted, anosmia may result.
Causes of anosmia range from the common cold to obstruction in the nasal passages by polyps or a tumor. Irritation of the nasal mucosa may result in temporary and partial anosmia, such as with acute sinusitis, the common cold, influenza, and nonallergic rhinitis. Tumors, polyps, or bony deformities of the nasal passages can cause permanent obstruction and result in complete and permanent anosmia. Anosmia may be a part of conditions like Alzheimer’s disease, Parkinson’s disease, multiple sclerosis, Sjögren’s syndrome, multiple system atrophy, and Huntington’s disease. Neurologic insults, such as traumatic brain injury, brain aneurysm, brain tumor, and diabetes, may also alter sense of smell.
Changes in olfaction may be a harbinger of safety concerns. For example, a diminished sense of smell and sensitivity to airborne chemical stimuli could put an individual at risk for missing the smell of smoke in the event of a fire or failing to detect a gas leak. Similarly, changes in olfaction may deleteriously influence nutritional intake; the inability to smell food and beverage aromas may lead to nutritional decline. Finally, changes in olfaction may lead to difficulty detecting food spoilage and the danger inherent in eating food that has spoiled. As with olfaction, age-related changes in taste do not inherently affect communication. However, changes in the ability to taste and to interpret taste have important implications for swallowing. These are discussed more fully in the dysphagia section of this chapter.
The decreased ability to taste certain types of foods is hypogeusia; the absence of taste entirely is ageusia. Dysgeusia refers to the presence of a metallic, rancid, or foul taste in the mouth. Most changes in the ability to taste have been attributed to a decreased sense of smell and the effects of various medications, diseases, chemotherapy, radiation therapy, and the use of tobacco. Diseases that alter smell and taste are more prevalent as people age. 15 Common changes in taste include a decreased ability to detect foods that are sweet. A diminished sense of taste may result in an inability to recognize spoiled food, which could result in serious illness.
In summary, age-related sensory changes can deleteriously affect communication across modalities and underscore the need for amelioration aimed at compensation. In terms of end-of-life care, these decrements in function warrant careful consideration. In the event that a patient needs to use a communication display or device but is without their glasses and possibly their hearing aids, the SLP needs to circumvent these issues by adjusting the font size and pitch and possibly rearranging some of the items to accommodate vision concerns. Without hearing aids, the patient may be disadvantaged when being instructed in use of a communication display/device, and the patient’s spoken communication with family members and medical personnel would also suffer.
20.3 Age-Related Changes in Communication
Age-related communication changes include alterations in voice and speech processes. Physiologic changes in the speech-production mechanism result in decrements in speaking rate, the presence of voice tremor, and changes in pitch and loudness. 16, 17 Voice changes related to aging of the larynx are known as presbyphonia and include the perception of increased effort to speak, vocal fatigue, difficulty with vocal projection, and altered voice quality. 18
Language skills are variably affected in aging: naming and comprehension of syntactically complex utterances may minimally decline, 19, 20, 21 whereas vocabulary, grammatical judgment, and repetition all remain relatively stable. 20, 22 Naming ability, particularly for nouns, is vulnerable to the ‘tip-of-the-tongue’ phenomenon that is common with aging and that can begin as early as the fourth decade; it becomes more prominent in the sixth and seventh decades. 19, 20, 23 Comprehension of syntactically complex utterances may be influenced by decrements in working memory capacity 24, 25 (see section on age-related cognitive changes). This is an important consideration in communication with both well and unwell elderly.
Age-related speech and language changes often occur gradually. In aggregate, however, sensory losses, particularly dual sensory loss, in combination with typical age-related language changes, can result in marked differences in communicative function. The sum of these changes can lead to psychosocial symptoms, such as social isolation, loneliness, and depression. 6
20.3.1 Communication Changes That Result from Terminal Disease Processes
Terminal disease processes and their sequelae can cause a range of communication changes with implications for the SLP. Many oncologic, neurologic, or neurodegenerative diseases can affect speech, language, and cognition and result in communication impairment. Although the nature of communication impairment differs across diseases, and even across the trajectory of a given disease, it is nonetheless a debilitating part of serious illness. Diminished capacity in a patient’s expressive and/or receptive communication abilities is referred to as communication vulnerability. 26 The concept of communication vulnerability is particularly apt in any discussion of communication at the end of life, since it encompasses the various changes wrought when serious illness interacts with communication across modalities. One of the very few constants in any disease process is change, and the concept of communication vulnerability is no exception to this rule.
A few major terminal diseases and their associated communication vulnerability are outlined below.
Head and neck cancers (HNC) can have profound effects on both speech and swallowing. Speech is directly affected in HNC that arise from mucosa lining the oral cavity, oropharynx, hypopharynx, larynx, sinonasal tract, and nasophaynx, 27, 28, 29 and from primary or secondary cancers of the brain. 30, 31 Owing to advances in medicine, many people with cancer are living longer after treatment. These cancer survivors may find that surgery and/or treatment result in changes in speech, language, cognition, and communication. 32 For some individuals, then, cancer is a chronic condition and the attendant communication issues may also be chronic.
The most typical speech changes that arise from HNC are dysarthria and/or dysphonia. Owing to the nature of surgical resection of these tumors, and the interdependence of anatomy and physiology in the speech mechanism, resumption of presurgery voice and speech may not be an option. 33 To achieve a semblance of communication naturalness, it is necessary to maximize residual anatomy and physiology. 18 In the case of partial glossectomy patients, the use of prosthodontic palatal appliances and articulation therapy may restore relatively natural-sounding speech. 34, 35 In contrast, for total glossectomy patients, palatal augmentation prostheses and articulation training have been less successful than other approaches in restoring speech naturalness. 35
For total laryngectomy patients, there are three primary options for voice and speech rehabilitation: (1) esophageal speech, (2) use of an electrolarynx, and (3) TE voice restoration. Many laryngectomy patients opt for use of the electrolarynx, since it is typically readily available in the postoperative period, provides access to voice, and is easy to use. Others reject the electrolarynx based on the mechanical sound of the voice.
Despite the best interventions, postoperative speech naturalness may not be satisfactory to some patients or their most frequent communication partners. Speech pathologists should consider, even during preoperative counseling, that the patient may need AAC as a permanent means of communication. 33, 36 The enormity of this change in communication method and the associated implications for quality of life cannot be underestimated. 37, 38 HNC survivors not only need to deal with the diagnosis, its prognosis, and potentially disfiguring surgery, but also need to live with significant alterations to quality of life that are wrought by limitations in the intelligibility of residual speech 28 and overall ability to communicate. 39
For some people, terminal disease processes are diagnosed in later adulthood. Others will age with a disease, and possibly a communication disorder, diagnosed in early to mid adulthood. This is the case with multiple sclerosis (MS), a chronic, progressive, neurologic condition that often yields changes in both speech and cognition. Though speech changes do not typically constitute presenting symptoms in MS, approximately half of the people with MS will have communication problems at some point during their disease. 40, 41, 42 The physical and psychosocial effects of MS, such as relentless fatigue and depression, compound the changes in communication status. 43, 44, 45 Changes in cognition, physical status, mental health, and speech can combine to escalate social isolation in this population. Furthermore, clinicians treating people with MS must keep in mind that the patient is aging with an existing communication disorder. The cumulative effects of aging plus a disability mean that the clinician may need to provide a spectrum of communication interventions over time to meet the needs of the patient with MS.
Parkinson’s disease (PD) may present both dysphonia and dysarthria, and hypophonia may be a presenting symptom in PD. In the early stages of the disease, speech and voice issues are amenable to change via behavioral therapy, the most widely known and researched being Lee Silverman Voice Treatment (LSVT). 46 As the disease progresses, however, LSVT may no longer meet patients’ functional communication needs. At that juncture, AAC options may provide the scaffolding for continued communication. 47, 48, 49, 50 Importantly, handwriting is rarely a means of either clarification and/or communication in PD, since micrographia (small handwriting) and intention tremor may interfere with the use of this mode of communication. Subsequently, the person with PD may need an expanded repertoire of AAC options to meet daily communication needs. These may include a voice amplifier and low- or high-tech communication aids to support communication across various environments.
Amyotrophic lateral sclerosis (ALS) is a rapidly progressive neurodegenerative disease. Although definitive diagnosis of ALS can be elusive and is still a diagnosis of exclusion, the most widely used diagnostic criteria are the El Escorial (Airlie Revision) criteria, in which the signs and symptoms are stratified according to clinical certainty. The three criteria are clinically possible ALS, clinically probable ALS, and clinically definite ALS. 51 When the disease announces itself with dysarthric and dysphagic symptomatology, it is referred to as bulbar-onset ALS. Patients who first present with weakness and/or atrophy in their extremities are said to have spinal-onset ALS. For these patients, dysarthria is likely to occur later in the disease process. In some instances, the clinical presentation contains elements of both bulbar- and spinal-onset ALS and is said to be mixed onset. Regardless of when the dysarthria appears or its severity, patients often rate communication issues as the most problematic part of ALS. 52, 53
The dysarthria most frequently associated with ALS is a mixed dysarthria, composed of elements of both spastic and flaccid dysarthria. 54 It is progressive and often terminates with a loss of useful speech. Hanson et al 55 completed a systematic review of dysarthria in ALS in which they described its characteristics, speech treatment, and AAC options. Evidence-based findings include the following: tongue and laryngeal impairments are common in ALS-associated dysarthria; even minor changes in intelligibility are associated with marked reductions of self-reported communication effectiveness; no literature-based support for effectiveness of exercise to strengthen oropharyngeal musculature exists, while literature-based support exists for limited use of prosthetic devices, such as palatal lifts or palatal augmentation devices.
Compelling literature exists attesting to the application and use of AAC options by people with ALS (e.g., Ball et al, 56 Doyle and Phillips, 57 and Fried-Oken et al 58). The use of AAC has gained the most traction with the ALS population owing at least in part to preserved literacy and the presumed preservation of cognition in this population. Further, because diagnosis of ALS is often made in midlife, when people are typically engaged in some type of employment, many people with ALS may be eager to continue their employment as long as possible. 59 Assistive technology (AT), of which AAC is a part, may facilitate the ability to continue to work as long as the burden of the disease allows. Research with the ALS population suggests that patients tend to use both low- and high-tech AAC options to meet their daily communication needs. Low-tech options, such as alphabet boards, communication displays, white erase boards, and paper and pen, may be used when speech intelligibility is in decline but high-tech options have not yet been explored or prescribed 57, 58, 60, 61 or they may be used throughout disease progression by people who prefer low-tech options. 62, 63 High-tech options, such as speech-generating devices (SGDs), are often prescribed for individuals with ALS and may provide significant assistance across communicative tasks and environments in which speech output is either required or desired. 64 Importantly, although low- and high-tech AAC options are sometimes addressed separately, it is their complementarity that often yields the most complete communication system for the person with ALS. Each is necessary and appropriate in certain situations. The ability to apply various AAC technologies as the situation warrants is a hallmark of a successful AAC user.
Although etiologies differ for each of the neurodegenerative diseases discussed above, and each has its distinctive neuronal signature, a systems approach is applicable when considering their communication aspects since they tend to share commonalities, in that each disease has a hallmark type of dysarthria, and they follow similar trajectories; namely, at disease onset most people are able to speak, and they progress to dysarthria, and some to anarthria, during the course of their disease. Each disease has an associated cognitive component that influences the window of opportunity in which to introduce AAC options (both low- and high-tech), followed by a cycle of ongoing education and intervention around communication issues. Furthermore, each disease has a disease-specific rating scale used in both clinical and research settings ( ▶ Table 20.1).
Disease | Clinical Rating Scale | Commonly Associated Dysarthria | Trajectory of AAC Use |
Amyotrophic lateral sclerosis (ALS) | ALSFRS-R | Mixed—spastic/flaccid | Bulbar onset— |
Multiple sclerosis (MS) | EDSS; MSRS-R | Ataxic and spastic | Intervene to educate re AAC; provide low-tech options and prescribe high-tech options as indicated. |
Parkinson’s disease (PD) | UPDRS | Hypokinetic | Early—voice amplifier |
Abbreviations: ALSFRS-R, ALS Functional Rating Scale (Revised); EDSS, Expanded Disability Status Scale; MSRS-R, Multiple Sclerosis Rating Scale (Revised); UPDRS, Unified Parkinson’s Disease Rating Scale. | |||
20.4 Age-Related and Disease-Related Changes in Cognition
A significant body of literature describes age-associated cognitive changes that, taken together, are referred to as cognitive aging (i.e., how cognition is altered in the context of presumably normal, healthy aging).
Although debate regarding causal factors continues, the following profile of cognitive aging has emerged: Older adults tend to have difficulty with episodic memory (i.e., conscious recollection of events), whereas semantic memory (i.e., accumulated world knowledge) tends to be preserved. Difficulty with episodic memory is manifested by poorer performance on learning tasks and in retrieval of both verbal and nonverbal material. Other areas of cognition that demonstrate fairly robust age-related changes are working memory, attention, processing speed, and task switching, all of which may be subsumed by the term executive functions. 65
20.4.1 Disease-Related Cognitive Changes
When cognitive aging goes awry, a spectrum of cognitive disorders emerges and pervades many aspects of daily life. The two main cognitive disorders addressed in this chapter are mild cognitive impairment (MCI) and Alzheimer’s dementia (AD), the most commonly known dementia.
MCI is a diagnostic entity that occupies a conceptual middle space between normal aging and AD. 66, 67 MCI encompasses a departure from normal aging in terms of cognitive status but does not meet the diagnostic criteria for dementia. MCI is characterized by memory impairment, with relative preservation of other cognitive domains so that normal daily functioning is not markedly interrupted. Subtypes of MCI include amnestic MCI (aMCI), which entails a primary memory deficit, multidomain MCI (md-MCI), which involves various degrees of impairment in multiple cognitive domains, such as language, executive function, and visuospatial skills, and occurs with (MCI +a) or without memory impairment (MCI –a). Less common is nonmemory domain MCI, which is characterized by impairment of a single nonmemory cognitive domain, such as language, executive function, or visuospatial skills.
Of note, people with MCI have an increased rate of progression to full-blown dementia when compared with their cognitively normally aging peers. 68, 69 Therefore, MCI is important both diagnostically and clinically. MCI may occur with other pathologies (e.g., PD) and may be developing in some patients who are referred for speech-language treatment near the end of life. A detailed history regarding memory complaints and descriptions of functioning across daily routines and environments that can be corroborated by an informant will help guide recognition of MCI as a clinically important variable in speech-language treatment.
In dementia of the Alzheimer’s type (AD), memory impairment is a hallmark of the disease. Physical aspects of the disease often occur later, when the disease process is already well established. Cognitive problems are broadly based, since it is memory, and primarily working memory, that is affected. Working memory girds other cognitive functions, such as attention, language use, and executive functions, all of which are affected in AD. 70 AD also affects noncognitive domains, such as social and occupational functioning. Therefore, AD’s effects are pervasive and inescapable.
The incidence of AD is increasing at an alarming rate, with predictions that it will reach epidemic proportions by 2050. A recent report indicated,
An estimated 5.4 million Americans have AD, including approximately 200,000 age < 65 years who comprise the younger-onset AD population. Over the coming decades, the aging of the baby boom generation is projected to result in an additional 10 million people with AD. Today, someone in America develops AD every 68 seconds. By 2050, there is expected to be one new case of AD every 33 seconds, or nearly a million new cases per year, and AD prevalence is projected to be 11 million to 16 million. Dramatic increases in the number of “oldest-old” (those age > 85 years) across all racial and ethnic groups are expected to contribute to the increased prevalence of AD. AD is the sixth leading cause of death in the United States and the fifth leading cause of death in Americans age > 65 years. Although the proportions of deaths due to other major causes of death have decreased in the last several years, the proportion due to AD has risen significantly. Between 2000 and 2008, the proportion of deaths due to heart disease, stroke, and prostate cancer decreased by 13%, 20%, and 8%, respectively, whereas the proportion due to AD increased by 66%.
The devastation wrought by AD on both speech and communication across modalities make it an important consideration for SLP assessment and intervention. Bayles and Tomoeda 72 have outlined the language impairment associated with AD, with loss of semantic memory being a cardinal symptom. In this regard, AAC offers specific options for the SLP working with persons with AD. External memory aids, such as memory books or remnant books or calendars, have been shown to help to structure access to memories and words 73, 74, 75 and to support conversation in individuals with moderate AD. 76
In addition to the physical aspects of neurodegenerative diseases like MS, PD, and ALS, there is also strong evidence for cognitive decline in each disease. Although the type and extent of the decline differ across diseases, it often occurs in addition to age-related changes, so its influence cannot be overestimated.
Cognitive impairment in MS varies from person to person and is tied to location, number, and activity of lesion sites. 77 Prevalence of cognitive impairment in MS ranges from 40 to 65%, 78 with evidence that the cognitive systems subserving memory, attention, and information-processing speed are the most commonly affected. 79
Cognitive impairment can occur at any point in the disease process. Once it begins, however, cognitive impairment is likely to continue along a slowly progressive course. 80, 81 Since MS is typically diagnosed in early to mid adulthood, changes in cognition, independent of physical disability, can have far-reaching implications for employment, everyday function, and quality of life. In a review of cross-sectional and longitudinal studies of cognitive changes associated with MS, Amato et al 80 reported that, based on magnetic resonance imaging (MRI) studies, cognitive deficits correlate with brain lesion burden and brain atrophy. Frontal lobe lesion burden has been associated with impairment in executive function, whereas involvement of subcortical white matter regions was associated with impairments in attention and memory. 80, 81 Cognitive changes in MS are associated with further decline, social isolation, and loss of , or cessation of, employment 82 but can be moderated by cognitive reserve. 83
In PD, cognitive impairment is widely recognized as a component of the disease process. Even in the early stages of PD, when motor symptoms tend to dominate, researchers have reported evidence of cognitive impairment. 84 As the disease progresses, the cognitive sequelae tend to worsen, although not always in tandem with the increasing severity of motor symptoms. 85 For approximately 30% to 50% of people with PD, cognitive function may deteriorate to the point where the diagnosis becomes PD with dementia (PDD).
The primary cognitive effect of PD is marked impairment of frontal/executive functions, 84, 86, 87 including inhibition, abstraction, attention, problem solving, reasoning, modulation of ongoing activity, working memory, and multitasking. Most, if not all, of these cognitive functions involve the frontal lobe. Thus, the anatomical relation between the frontal lobes and the basal ganglia provides support for the role of the frontostriatal circuitry in the cognitive dysfunction in PD. Significant evidence also exists to support a working memory deficit in PD, with visuospatial working memory being more affected than verbal working memory. 88
ALS was once thought of as a purely motor disorder, but research indicates it has a cognitive component in 15 to 40% of cases. 89, 90, 91, 92 The cognitive impairment associated with ALS is a form of frontotemporal dementia (FTD) that yields early and observable changes in behavior, executive function, and language. Cognitive change may precede the onset of physical symptoms, although there are certainly instances in which the onset of both co-occurs or the physical ALS symptoms precede the FTD changes. Patients with ALS who also have cognitive impairment tend to have shorter survival times. 93, 94
Unlike the memory impairment that typifies AD, memory is generally intact in FTD. The behavioral variant of FTD (bvFTD) includes three subtypes that are differentiated by primary presenting features: (1) a disinhibited type, which manifests lack of judgment, frequent swearing, impulsive buying, paranoia, delusions of grandeur, and sometimes criminal activity; (2) an apathetic type that manifests as blunted emotions, overarching apathy toward everything and everyone, lack of empathy, and lack of attention to personal hygiene; and (3) the stereotypical type that manifests as hoarding, overeating, and repetitive behaviors.
The language changes that accompany FTD include three possible types: (1) primary progressive aphasia (PPA); (2) nonfluent progressive aphasia (NFPA), which is characterized by relatively preserved comprehension in the face of growing difficulty with language expression, independent of any motor speech component, and anomia, phonemic paraphasias, oral apraxia, alexia, and/or agraphia may all be present; (3) semantic dementia, which is characterized by fluent speech replete with anomic errors. Thus, speech is fluent but void of content, and comprehension is typically impaired as well. Executive dysfunction is very common in FTD and is manifested in problems with planning, strategizing, organizing, and abstracting. Verbal fluency is often markedly impaired in FTD.
It is unclear whether the cognitive impairments associated with MS, PD, and ALS affect the patient’s ability to learn to use assistive technologies, including AAC. However, the involvement of executive function across diseases and its importance in learning suggest that cognitive impairment has the potential to affect both initial learning and ongoing use of AAC. Early work in this regard suggests ways in which the cognitive impairment in ALS may influence use of AAC and how to mitigate some of the effects of cognitive decline on use of AAC. 95
Further, the fact that shorter survival times are associated with cognitive impairment in ALS suggests that it is important to identify its presence as early as possible. If AAC intervention is undertaken early enough and the patient can learn to use an AAC system (either low-tech, high-tech, or both) to a level of high familiarity it is conceivable that the ability to use the system will be retained for the duration of the disease.
See ▶ Table 20.2 for a summary of the neurodegenerative diseases, the associated cognitive components, and the implications for use of AAC.
Disease | Associated Cognitive Impairment | Characteristics of the Cognitive Impairment | Implications for Use of AAC |
Multiple sclerosis | Frontal lobe symptoms | Variability depending on location of lesion; memory issues, slowed information processing, attention deficits, issues with problem solving | Various AAC options at appropriate times; focus on energy conservation and efficiency. Visual problems may limit use of AAC. Cognitive issues may affect learning to use AAC system(s). |
Parkinson’s disease | Parkinson’s disease dementia (PDD) | Executive dysfunction, delusions, hallucinations | Various AAC options at appropriate times; voice amplifier when LSVT no longer viable; high-tech AAC options as indicated. Tremor and cognitive decline may make alternate access necessary. |
Amyotrophic lateral sclerosis | Frontotemporal dementia (FTD) | Executive functions impaired; attention deficits, decreased speed of processing | Introduce AAC options early; will need to rely on procedural memory. |
Alzheimer’s disease | Dementia | Memory (primarily working memory), executive function, and language | Introduce AAC options early; stress low-tech options (e.g., remnant books, visual schedules) |
For all of the above, the preservation of procedural memory is what supports learning to use AAC options. LSVT, Lee Silverman Voice Treatment. | |||
20.5 The Role of the Speech-Language Pathologist in Providing Communication Services to People at the End of Life
SLPs play an important and expanding role in service provision to people at the end of life 96, 97, 98 across a spectrum of care environments—home, hospital, hospice, long-term-care
facility, and nursing home. 99 Although time horizons may be short and disease processes may be advancing toward their inevitable conclusions, SLPs can provide options for maintenance and/or amelioration of communication (either vocal, written, or with the aid of some type of communication augmentation). Treatment goals should be to meet the patient’s needs and to provide a means of communication for the remainder of the patient’s life. The goals of treatment in this phase are twofold: (1) to provide communicative palliation and (2) to attenuate the effects of communication vulnerability brought on by aging, serious illness, trauma, and severe cognitive decline, or some combination of all four.
It is neither easy nor straightforward to incorporate the above into end-of-life care. One option available to SLPs is to set their treatment goals using the method of goal attainment scaling (GAS). 100, 101 GAS allows for evaluating individual progress toward goals when goals are framed with a continuum of five possible outcomes and are weighted from negative two to positive two. The five possible outcomes range from worst expected outcome, to less than expected outcome, to expected outcome, to more than expected outcome, and best expected outcome. In this way, clinicians are not forced to evaluate progress against a single metric (e.g., 85% accuracy) with the added benefit that performance can be measured at treatment outset, intervention can occur, performance attained for each objective can be determined, and evaluation of overall goal attainment can follow. This is a useful model for end-of-life care, when the intended outcome is not skill improvement, but instead is having the individual be able to communicate within desired and obligatory contexts even when initial performance and prognosis are both poor.
Ideally, SLPs should be involved in an interdisciplinary care team throughout a patient’s care, or at least should be consulted at multiple points along the way. SLPs may be integral in determining cognitive capacity, providing important input regarding nutrition and hydration, and in providing education, counseling, and access to communication options and strategies. Thus, the SLP should not be relegated to a one-time consult, but should become part of the fabric of the continuum of care.
Although direct service may be provided to the patient, SLPs typically also provide education to other team and family members, and provide counseling about communication and swallowing issues. These services complement one another; direct service may stand alone, but everyone involved benefits when education and counseling are an integral part of service provision.
Provision of services to people at the end of life hinges first and foremost on the SLP’s understanding of, and comfort with, issues surrounding death and dying. As the population ages, and an ever-increasing cohort of elders presents with end-of-life issues, SLPs will need to prepare to meet the needs of this varied population. 102
Issues surrounding death and dying need to be addressed during the SLP’s preprofessional training. Graduate students need to be aware that no clinical setting or population is exempt from the possibility of patients’ dying; tragic accidents can happen at any time to anyone, acute or chronic illness can claim children and adults alike. The enormity of this existential issue requires sensitivity when it is presented to students. Not all students in preprofessional training programs will have personally experienced the death of a close friend or relative. Therefore, students must confront death from their own personal, cultural, and religious beliefs before they can fully consider death from the perspective of the patient and his or her family. Thus, education must specifically address the clinician’s professional roles, responsibilities, and specific duties as they relate to the dying patient. 67, 97, 98 This information is important in preprofessional preparation because it influences both the timelines and the types of SLP services that may be needed.
Models of grieving (e.g., Kubler-Ross, 103 and the new grief described by Okun and Nowinski 104) can be presented within the counseling curriculum and/or infused into the curriculum at appropriate junctures, ensuring that all students are exposed to the material prior to graduation. The Kubler-Ross model 103 has been a mainstay of education about death and dying. This model hypothesizes that there are five stages through which most people pass when they know they are dying or if they are grieving a significant loss. The stages are denial, anger, bargaining, depression, and acceptance. Importantly, passage through the stages is not linear; rather, they can overlap, and each person experiences the progression at his or her own pace.
In contrast to the Kubler-Ross model, Okun and Nowinski 104 predicate their five-stage model of family grief on the fact that medical advancements have, in large part, transformed death from an event into a process. Even a terminal diagnosis does not always signal imminent death; in many instances, patients and families may have months or years to deal with a loved one’s illness and pending death. The stages of the Okun and Nowinski model are crisis (receiving a terminal diagnosis), unity (coming together to support the dying person and to meet their growing medical needs), upheaval (the stage in which the ongoing and increasing needs of the dying family member begin to extract a heavy toll on those providing care—their lives have significantly changed, and they continue to watch their loved one deteriorate), resolution (acknowledgment by all that the ill family member is, indeed, dying, and that it is helpful to resolve unfinished business so that the remaining family members can bond and support one another), and, finally, renewal (which begins with the funeral or celebration-of-life ceremony; it includes sadness about the loss but also allows for relief that the suffering is over, and each family member as an individual, and the remaining family members as a whole, can seek renewal and redefined family traditions).
An example of implementation of a focused palliative care curriculum for speech-language pathology students met with significant success. 105 In this program, students received direct instruction and opportunities for self-directed learning in the process of “palliative thinking.” Although results of this one program cannot be generalized across all SLP training programs, as a profession we need to consider how to address personnel preparation for the palliative work incumbent on many SLPs. 96, 99, 106 Indeed, as a profession, speech-language pathology may draw upon a wealth of information and palliative care training options that are based in medical and nursing education (e.g., Block 107; Downe-Wamboldt and Tamlyn 108; Billings et al 109; Sanchez-Reilly and Ross 110; Bays et al 111).
To complement the above, students should be exposed during their graduate careers to the cultural spectrum inherent in the concept of disablement. 112 Briefly, “disablement refers to the effects that chronic and acute conditions have on the functioning of specific body systems and on people’s abilities to act in necessary, usual, expected, and personally desired ways in their society.” Although a thorough treatment of this topic is beyond the scope of this chapter, readers are encouraged to consider that disablement is a process that occurs across time. Its nature can fluctuate according to the changes in functional status imposed by illness. This sociological construct is extremely informative and valuable when considering end-of-life issues.
Disablement, as viewed through various cultural lenses, is intimately bound up with end-of-life issues. The cultural influences may interface with patients’ and families’ willingness to accept and/or engage in speech and language intervention. SLPs must be knowledgeable about the nuances of how culture interfaces with ideas about illness, death, and dying. 113, 114
A related concept is cultural humility, 115 which refers to the values and attitudes that health care providers need to cultivate in their work with patients. It involves a sincere motivation to understand the culture and meaning in which children and families live, and the reflective capacity to examine our own cultural values and assumptions. This concept entails meeting the patient and family “where they are” and allowing their opinions and concerns to be fully heard and valued in the decision-making process. Cultural humility is critically important when medical knowledge, authority, or convention may run counter to a patient’s and/or family’s wishes.
20.5.1 Strategies for Facilitation of Communication at End of Life
Use of AAC at the End of Life
As a group, investors tend to be historians and not futurists, predicating financial decisions on past performance of investment vehicles or stocks. In many ways, SLPs have approached the planning of vocabularies for low- or high-tech AAC systems for terminally ill patients in much the same way, using information regarding the patient’s personal and family history and past events to inform vocabulary selection. This is not trivial, because it is an important part of working with a patient at the end of life, however, it is also critical to provide vocabulary for communication about events related to the person’s present illness, death, and dying. Comprehensive planning includes giving the patient a way to talk about future events that may occur after his or her death. For instance, people need a way to communicate about their impending death in both its physical and spiritual dimensions, grief and mourning, planning a funeral, contributing to or composing their own obituary, family occasions for which they will not be present (both in the near and distant future), and their future wishes for family members, friends, pets, etc. (e.g., for a spouse—“I hope that you will remarry one day and be happy”; for a child—“I wish I could be there for every event, big and small, in your life. I will miss being physically present at your graduation, your wedding, and the birth of your children, but I will be with you in spirit.”).
A significant body of literature supports the use of AAC in intensive care units (e.g., Garrett et al 116; Happ et al 117; Menzel 118). In some cases, AAC is used temporarily to help people who are unable to speak because they are mechanically ventilated, while for other people use of AAC may be more permanent (e.g., someone with end-stage neurodegenerative disease who has lost the ability to speak). In all cases, the role of the SLP is to facilitate communication. 99, 119, 120
A number of protocols exist for implementing AAC options to facilitate communication at the end of life. The use of AAC in pediatric palliative care is well documented. 26, 121 The Children’s Hospital Boston model stresses both pre- and postoperative care and counseling regarding communication whenever possible. Preoperative care can mitigate some of the fear that occurs when a patient finds he or she is no longer able to speak. The model emphasizes the importance of ongoing assessment and system revision to meet changing needs. These same principles, although outlined for use in a pediatric setting, can be readily applied for use with patients of all ages. Attention to patients’ ability to communicate is vitally important, particularly in diseases where the prognosis is poor and patients may be in various stages of dying. 122
Message banking is a way for people to digitally save spoken messages that vary in length from words to phrases to longer narratives. These messages can then be uploaded to a communication device and/or saved on a CD or MP3 player or mobile tablet. When the nature of the pathology allows time to engage in this activity while the speaker’s speech is viable, message banking is a powerful way for the patient to leave a vocal legacy. 57, 123, 124 Using banked messages on a communication device provides a vehicle for personalizing the prosody and the communication. Users can opt to use synthesized speech for routine messages and their own banked speech for more personal or important messages. Apps for mobile tablets that support message banking and/or storytelling allow the patient to pair message banking with pictorial elements, yielding a multimodal legacy.
Low-Tech AAC Options and Techniques
Fried-Oken and Bardach 125 reported on five themes identified as the most important end-of-life issues for extant AAC users: range of AAC options, techno-connectedness, the importance of communication partners, quality of life, and quality of death. These five issues were culled from quotes of people who use AAC and related to how AAC may be a vital part of facilitating and maintaining social closeness, allowing for discussion about one’s wishes regarding quality of life and quality of death, and having access to the AAC options to participate in daily communicative opportunities. Balandin and Morgan 126 surveyed 270 adults with cerebral palsy and found that their concerns included health maintenance and continued access to effective communication options and services as they aged. Aging and AAC use are intricately bound together; one does not preclude the other, and many people may find increased reliance on AAC tools and technologies as they age and approach the end of life.
SLPs use information regarding a patient’s illness and prognosis to plan intervention to support communication at the end of life. Ideally, it is best to have AAC options in place before the burden of disease increases exponentially and speech is no longer a viable means of communication. However, in the case of sudden illness or injury, or emergency surgery from which the patient emerges unable to speak, AAC options must be implemented to facilitate communication with loved ones, medical personnel, and care providers. When there is an emergent need for AAC, low-tech solutions can often be implemented quickly and efficaciously. There is an ever-increasing range of available low-tech AAC options. Some are commercially available in mass-market outlets (e.g., electronic magic erase boards, white erase boards), and some are commercially available online (e.g., prefabricated communication displays). Using readily available items, such as a notebook and pen/marker, the clinician can demonstrate how to use written choice conversation (e.g., Lasker et al 127) with someone who, for whatever reasons, can read but cannot write. This technique involves presenting the person unable to speak with written multiple-choice type questions/options structured with easy-to-understand, topic-relevant language and clear visual presentation. For instance, when presenting a question regarding a visit by a cherished family member, the written choice communication might be modeled as follows:
Clinician: How was Janie’s visit?
Clinician then writes choices: not so good, okay, good, great
Patient then points to desired response. Clinician continues the conversation by asking:
Clinician: What did she tell you about the baby?
Clinician then writes choices:
He’s teething
He’s crawling
He’s sleeping through the night
Clinician: The baby is crawling already! Bet he’s into everything. Did she bring pictures?
Patient indicates yes/no with facial expression or gesture.
Clinician/communication partner can develop this thread to allow conversation to unfold in a more naturalistic manner.
Once low-tech systems or options are in place, the clinician’s role is to then customize commercially available options for the individual patient by
Adding personally relevant vocabulary/phrases to make the communication technology more user-friendly.
Providing instruction in its use to patient, family, and friends, as well as members of the patient’s medical team.
Adapting access so that something designed for use via direct selection may be used with an alternate form of access (e.g., with a side-mounted head light or with partner-assisted scanning).
If warranted by the patient’s clinical reality, the clinician can also prepare patients and all members of their team for growth of the AAC system to include high-tech options.
Low-Tech AAC Techniques to Enhance Speech Intelligibility
Speech or alphabet supplementation—the patient continues to use speech but supplements the spoken output by pointing to the first letter of each word spoken on an alphabet display. Speech supplementation provides benefits for both speaker and listener. For the speaker, it allows the patient to continue to use natural speech but to cue the listener for each spoken word, thus diminishing the effect of long streams of severely unintelligible speech. For the listener, it decreases the need to ask for repetition of the spoken message and the ensuing frustration of being in a conversation where the message can be lost in the effort of trying to convey it. This method tends to work best for severely dysarthric individuals. 128
Topic or semantic supplementation—the patient continues to use speech but supplements the spoken output by pointing to a topic word that will cue the listener by providing the topic of the about-to-be-spoken message or messages. This may be done on a communication board or may be written out by individuals who retain their ability to write. Cuing a communication partner in this way constrains the context of the pending conversation and steers the communication partner toward semantically relevant ideas and vocabulary. Topic supplementation can be paired with speech/alphabet supplementation to yield enhanced intelligibility. 128
Although speech and topic supplementation are not the only techniques to enhance speech intelligibility, they are relatively easy to demonstrate and to teach within the context of the patient receiving end-of-life care. Family members can be trained to verbally or gesturally cue the patient to provide the necessary information, to confirm with the patient that the intended information has been conveyed by repeating the letter(s) and/or topic(s) chosen, and to reinforce its utility by engaging in the conversation the patient desires, rather than constantly asking for repetition, which increases frustration and blocks effective communication.
Important Issues in Implementation of Low-Tech AAC Options and Strategies
Exigencies of time—In both emergent and end-of-life situations, communication must take place expediently so that important decisions can be made with the patient’s input. Ensuring the patient has a way to communicate, even when it does not include speech output, is critical in allowing care and decisions regarding care to proceed with minimal disruption. (See also the above discussion of the range of technology.)
Keep it simple—Low-tech options that require minimal instruction in their use are likely to facilitate expedient communication in both emergent and/or end-of-life situations. These options include, but are not limited to, items like electronic magic erase boards, white erase boards, notepads and pens/pencils, prefabricated communication displays, alphabet boards, and speech/topic supplementation.
Cognitive considerations—In the event that cognition is compromised to the point that spelling is not reliable, the use of pictures/photos can be helpful. Some prefabricated communication displays come in text and/or picture versions and can be helpful in this situation. Likewise, photo albums provided by family members can be used to elicit communication and to evoke memories.
20.5.2 Bridging the Gap Between Low- and High-Tech Options
Assessment for high-tech intervention (e.g., for an eye-tracking speech-generating device) is a time-intensive process and may not yield immediate results for the user. However, when the opportunity exists, the skilled clinician can provide information about, and access to, high-tech AAC options.
Mobile tablets and/or smartphones—Many patients are active consumers of current technologies, and they may already be using these platforms to communicate via text messaging, email, talking on the phone, and/or videoconferencing and the like when they reach the end of life. These technologies lend themselves to continued use when appropriate supports are available. Mobile tablets and the apps that run on them were designed for use via direct selection (i.e., ability to use a touch screen and onscreen keyboard). If a patient were to require alternate access due to physical limitations (i.e., the patient cannot use a touch screen and onscreen keyboard via touch and/or stylus), a platform that supports the patient’s needs needs to selected. At the time of this writing, the Android platform supports alternate access more fully than the iPad does, although developers are working to ensure that all major mobile tablet platforms become accessible via multiple options. There are, however, switch options for the iPad to facilitate use of certain apps. The caveat being that although certain apps may be supported to work via alternate access, the operating system (iOS) is not. There are many options for communication apps, and more are being developed all the time. Careful assessment via feature matching 129 by an SLP and possibly an occupational therapist will facilitate a patient’s continued access to his or her device, when possible. With the addition of communication apps to support speech output (either via text-to-speech or via symbols) or speech-recognition input for writing (if possible), an existing technology can meet previously unanticipated needs.
Providing a way to map existing communication skill/abilities onto a system that provides additional capacity—When an individual is already using a communication system (gesture, pen and paper, an electronic magic slate or a tablet), it is important not to overwhelm the patient and family with options. This is particularly important when sudden illness or trauma has rendered the patient unable to communicate via natural speech. Most people want to use speech as their default mode of communication. Accepting that speech is no longer optimal as a way to meet daily functional communication needs is a process that takes time. To facilitate transition to use of additional AAC options when speech is not adequate, this chapter’s first author (MLG) has found it helpful to demonstrate how to use whatever native mode of communication remains and how to add just one step using AAC. For instance, if the patient can no longer speak but can write with a nondominant hand due to severe weakness of the dominant hand, adding in the ability to type on a tablet with a speech output app gives the patient the option of using typing and writing to gain access to speech output. This holds true even if typing is hunt and peck rather than rapid and fluid. In another example, giving a voice amplifier with a lapel microphone to someone who is extremely hypophonic allows them to use their existing speech but amplifies the output so that it is audible to listeners. Moving beyond this initial foray into assistive technology takes time, effort, and expertise. Facilitating buy-in can be mediated by this step-by-step approach.
Despite the heterogeneity of illnesses and conditions that may result in end-of-life care, communication vulnerability is a common thread among them. The SLP can intervene and provide much-needed support at this juncture in a patient’s care so that the patient can communicate and participate in medical decision making. Goals of care are to lessen the burden of communication vulnerability by providing compensatory strategies, which may include AAC options. As the population ages, and the cohort of elderly, both well and unwell, increases in size, the demand for quality SLP intervention as part of end-of-life care will increasingly drive both personnel preparation and service-provision mandates.
20.6 Swallowing Issues and the End of Life
Issues with swallowing near the end of life may arise due to the progression of neurologic disorders resulting in dysphagia as well as due to the physiology of dying related to acute or chronic illness, injury, or advanced age. The typical graduate curriculum prepares students to work toward the rehabilitation of the dysphagic patient, but most students are not trained in the area of end-of-life management of swallowing disorders. A review of the literature and the guidelines established by ASHA make it clear that SLPs have a place in this arena as a member of a multidisciplinary team. 99, 130, 131 This section of the chapter discusses the effects of aging on swallowing function, the specific changes in swallowing in patients with dementia, approaches to evaluation and management of dysphagia at the end of life, physiologic changes that occur in the dying process, perspectives on alternative nutrition and hydration, and the team approach. Finally, we present illustrative cases that encompass common experiences in managing dysphagia at the end of life.
20.6.1 Age-Related Physiologic Changes That Influence Swallowing Status
The aging swallow is characterized by alterations in sensory and motor functions, and these changes are well documented in the literature. 132, 133, 134, 135, 136 The challenge for the practicing clinician is distinguishing between the changes in eating and swallowing function associated with normal aging and the effects on eating and swallowing brought on by diseases and disorders prevalent in the elderly, such as stroke, transient ischemic attacks (TIAs), progressive neurologic disorders, arthritic changes to the cervical spine, vascular changes, hypertension, diabetes, lung disease, and cognitive changes due to dementia. In addition, the polypharmacy that is often characteristic of care for older individuals can cause medication-related effects on the physiology of eating and swallowing. ▶ Table 20.3 lists some of the changes that occur in normal aging that can affect swallowing.
Oral Phase | Decreased tongue mass |
Poor dentition | |
Gum atrophy (poor fitting dentures) | |
Pharyngeal Phase | Reduced strength of pharyngeal constriction |
Prolonged pharyngeal transit time | |
Increased incidence of cervical osteophytes | |
Reduced posterior pharyngeal wall mass with increased pharyngeal space | |
Increased incidence of cricopharyngeal bar | |
Decreased duration of upper esophageal sphincter opening | |
Esophageal Phase | Reduced esophageal peristalsis |
Elderly individuals may deny eating or swallowing problems but on further questioning will acknowledge that they take greater care when eating by taking smaller bites, chewing more thoroughly, and avoiding foods that are difficult to chew. They may also report the need to swallow repetitively or to “wash food down” with liquids, and they may avoid eating out due to coughing or “strangling.” Changes and adaptations occur gradually, so elders may not perceive them as problems. However, age-related changes may represent dysphagia risks in the elderly, and the risks can be exacerbated during acute and/or terminal illness.
As clinicians working with the elderly, SLPs who understand these changes have options for minimizing swallowing difficulties related primarily to aging. There are several potential interventions that can enhance the sensory input of foods. Increasing the variety of textures and creative seasoning in foods can increase palatability. Ensuring appropriate serving temperatures can increase swallow responsiveness. When oral intake is diminished, consultation with a dietitian can provide strategies to maximize nutrition density per quantity of intake.
Improvement in eating and swallowing function in the elderly can be facilitated through indirect and direct interventions. Indirect interventions include education regarding the importance of good dental and oral health, developing strategies for “social” eating or pleasure eating with others, and teaching precautionary measures, such as early airway closure and repetitive swallow. Direct interventions include using exercises to increase lingual pressure and upper esophageal sphincter (UES) opening 137 and respiratory strengthening exercises. 138
20.6.2 Influence of Dementia on Swallowing Function
Physiologic changes contributing to dysphagia in the patient with dementia can confound and amplify the typical changes due to aging. Xerostomia due to medication effects and decreased fluid intake are significant concerns. In the oral stage, there can be decreased lateral tongue movement, while in the oral pharyngeal stage of the swallow, there can be reduced lingual retraction, diminished laryngeal elevation, and bilateral pharyngeal hypomotility. 139
Physiologic swallowing deficits in dementia are affected by deterioration in cognitive/communicative abilities (memory, judgment, abstract reasoning, and language), motor function (apraxia), and sensory functions, all of which can result in feeding challenges over and above dysphagia. Agnosias (for food substances and taste) have been reported, along with alterations in taste (dysgeusia or ageusia). Patients with dementia can have apraxia of feeding, which is characterized by overfilling of the mouth with food or liquid as well as eating nonedible objects and pilfering any food or nonfood items within reach. In general, cognitive impairment in attention, planning, conceptualization, visualization, and initiation will affect the eating process. Patients can often forget that they’ve eaten and may not respond to internal feelings of satiety or may present with decreased appetite. In later stages of dementia, loss of language skills can impede letting caregivers know that they are hungry. 140 See also Chapter 6 for a comprehensive overview of cognitive and behavioral changes in dementia.
In general, dementia results in an overall slowing of the swallowing process. This motor slowing continues as the disease progresses and leads to mealtimes that are longer, increased risk for aspiration because of slowed pharyngeal response and airway exposure, and an increased dependence on others for feeding, the latter being a risk factor for aspiration pneumonia. 141
20.6.3 Evaluating Dysphagia at the End of Life
Often, an early step in the continuum of care is a physician referral for swallowing evaluation. In some cases, a clinical swallowing evaluation may be ordered when a patient is delirious or poorly responsive and is thus unable to participate in a full evaluation. In that case, screening a patient to assess safety is appropriate. This can also create an opportunity to begin counseling families. Education regarding the effect of altered mental status on swallowing safety is critical, especially when families are concerned that their loved one is not eating. They might voice concern that the patient is starving to death. Gentle discussion about physical changes at the end of life can promote the understanding that the body does not require nutrition as it is shutting down, that changes to the brain diminish the sense of hunger one might feel if healthy. This discussion might include a shift in paradigm; the patient is not dying because he or she is not eating, but because they are at the end stage of life or of a terminal disease process. This will permit families to shift their attention from maintaining nutrition to making the patient comfortable.
Instrumental swallowing assessments are valuable for determining the safest diet consistency and swallowing or feeding strategies, whether the person will only eat for “pleasure” or chooses to continue full oral nutrition despite documented risk for aspiration. Groher and Groher 142 provide an excellent review of the role of the modified barium swallow study (MBS) at this stage of life, describing the importance of a repeat MBS if a known aspirator chooses to continue eating, indicating that reassessment should focus on the “swallow-safe” bolus to determine the patient’s ability to swallow materials with the least amount of aspiration. This might mean testing a full array of textures, volumes, and delivery methods. The emphasis of the assessment and interpretation should be on the aspects of swallowing that remain strongest. The intent of the evaluation is to determine whether existing strengths might be enhanced by changes in the bolus, method of presentation, or postural changes.
In some cases, families do not wish to subject the patient to significant testing and may decline instrumental assessments. It is the clinician’s responsibility to inform them of the benefits and limitations of each assessment as well as the risk for aspiration and potential pneumonia so they can make informed choices. Documentation should reflect the date, discussion specifics, patient or family acceptance or refusal of the information, the patient’s goals and wishes, as well as the risks and benefits of a given treatment plan. In addition, it is essential to document the education provided regarding specific food or liquid texture modifications and/or compensatory strategies for safest feeding. Indicating the type of information, verbal and/or written, and the need for continued education in the case of limited understanding or poor acceptance of the information, will confirm fulfillment of the physician’s order in the medical record. According to Levy et al, 143 it is also helpful to document specific patient and family statements and to refer to physician documentation of “do not resuscitate,” “no code,” or “no tubes.” Specific orders may also be written, such as, “Per patient wishes, he/she is allowed to take an oral diet.”
When a patient elects to eat or drink despite clear risk of aspiration and respiratory infection, some facilities require that an informed consent be signed and placed in the medical record. The SLP must understand the facility’s policy and adhere to it. The SLP should clearly document that the patient and/or surrogates were fully informed of the continued risk and potential consequences of oral alimentation. Some clinicians might be uncomfortable providing education regarding continued oral intake in such cases or believe that their ethical standards are threatened; in that event, they have the right to pass the case on to a colleague who does not feel that their personal or professional ethics are compromised by such involvement. 144 Continued involvement in the case will allow for reassessment and continued discussion during periods of change, with the possibility that the patient or caregivers may alter their original decision.
20.6.4 Management of Dysphagia at the End of Life
Treatment considerations when addressing the swallowing issues of the patient at the end of life should include the basic principles of quality of life, dignity, and comfort. Management should include environmental modifications, increased mealtime supervision and cueing, diet modifications to include sensory enhancement, and increased availability of nutritious snacks and drinks provided over the course of the day. Periodic swallowing assessments may be necessary to allow adjustments in the treatment plan to correspond with the progression of dysphagia.
Alternative Nutrition and Hydration
When a patient is unable to obtain adequate nutrition and hydration orally, these requirements can be delivered either through either enteral or parenteral nutrition. Enteral nutrition delivers prepared high-calorie formulas to the feeding site by nasogastric (NG), gastrostomy (PEG or G-tube), or jejunostomy (J-tube or PEJ). The formula may be delivered continuously from a plastic bag by a pump over an extended period of time or it may be hand-delivered from a syringe into the tube (bolus feeding). NG tubes pass through a nostril into the pharynx, through the pharyngoesophageal segment into the esophagus, and through the lower esophageal sphincter into the stomach. If gastroesophageal reflux is a concern, or if the stomach is compromised, the tube is passed through the pyloric valve into the jejunum. NG tubes may also be used to suction secretions pooled in the pharynx in cases of poor secretion management or to measure residual stomach content. Dobhoff tubes (DHT) are smaller and weighted at the distal tip for easier insertion but are more prone to clogging. Patients may consider NG tubes to be uncomfortable and may complain of a sore throat. NG tubes are generally considered a temporary means of alternative nutrition when the medical team expects a short recovery period of 3 to 4 weeks or wishes to “buy time” for medical decision making. NG tubes are generally placed at bedside and checked radiographically to ensure appropriate positioning in the digestive tract.
Gastrostomy and jejunostomy feeding tubes are considered to be more permanent but reversible means of artificial nutrition and may be placed surgically under general anesthesia or endoscopically (PEG or PEJ) with light anesthesia. When the stomach must be bypassed and the tube is placed in the jejunum, a more specialized predigested formula must be used.
Parenteral nutrition is delivered directly into a central vein, such as the subclavian or internal jugular vein, when the gastrointestinal tract is nonfunctional due to bleeding, gastroparesis, or obstruction. Total parenteral nutrition (TPN) provides a specialized formula and may be used for 4 to 6 weeks. 145 Peripheral parenteral nutrition is delivered through a peripheral vein primarily for hydration or the delivery of medications, as with an IV. This method is generally effective for 7 to 10 days. 145
Hypodermoclysis is a means of supplementing hydration for mild to moderate dehydration. A half saline/glucose (potassium chloride may be added) injection is given subcutaneously in specific sites, such as the chest, abdomen, thighs, and upper arms. This method is considered safe, with the most frequently occurring adverse reaction being mild subcutaneous edema. 146
Often, families may direct questions regarding alternative nutrition and hydration (ANH) to the SLP. SLPs should be prepared to discuss the specific implications of, and erroneous assumptions about, using ANH in this population. Often, professionals as well as families have several beliefs about the utility of ANH. Common beliefs about percutaneous endoscopic gastrostomy (PEG) tubes are that they (1) prevent aspiration, (2) prevent malnutrition, (3) prevent pressure ulcer formation and promote healing, (4) improve overall functional status, (5) improve quality of life, and (6) improve survival. Galicia-Castillo and Martin 147 dispel these common assumptions.
Aspiration prevention—There are no data supporting the claim that PEG tubes will decrease the risk of aspiration from regurgitation of gastric contents 148; orally fed patients had significantly less aspiration than tube-fed patients. 149
Malnutrition prevention—The long-term effects of chronic disease, immobility, and neurologic deficits may undermine attempts at long-term nutritional support. 150
Pressure ulcer prevention—Finucane et al 150 reported data linking malnutrition and pressure sores were incomplete and contradictory; they concluded that the data do not support routine use of tube feeding to prevent or heal pressure sores.
Functional status improvement—Retrospective review of data demonstrated no improvement in functional status as measured by the Functional Independence Measurement (FIM) scale during an 18-month period after PEG placement. 151
Quality of life improvement—The presence of PEG tubes may result in local complications, such as pain, suture breakage, cellulitis of the abdominal wall, abscess of the abdominal wall, stomal inflammation, skin excoriation, bleeding from the site, closure or stenosis of the stoma and hematoma, agitation due to use of restraints, pleuropulmonary complications due to erosion of the tube into the pleural cavity, gastric perforation, abdominal discomfort, mechanical malfunction and accidental dislodgment, and the loss of the social aspects of oral feeding. 147
Increased survival—Inability to eat orally marks the final stages of dementia, the median survival rate after PEG placement is 7.5 months. 148 For patients who survived more than 60 days after nasogastric tube (NGT) placement, 70% had no significant improvement in nutritional, functional, or subjective health status. 152
As a member of the multidisciplinary team caring for patients with end-stage dementia, SLPs can assist family members and surrogate decision makers by first understanding their motivation and goals for the patient before educating them regarding the clinical evidence. Use of an algorithm for decision making in determining whether to recommend tube feeding can be helpful. The algorithm proposed by Rabeneck et al 153 provides comprehensive guidelines for PEG placement in all patient populations and is based on the reason for PEG consideration.
If the patient has an anorectic-cachectic syndrome, the option of PEG tube placement is not offered, since the patient is most likely unable to utilize the nutrients it would provide. If the patient is in a permanent vegetative state, the SLP may recommend against PEG, since it is unclear whether the patient may experience any improvement in quality of life. For the patient with dysphagia without other complications, the SLP may recommend a PEG tube, since the patient is most likely to benefit from its use. In the case of dysphagia with complications, the SLP should offer a discussion regarding trial versus no trial of PEG tube use, since it is unclear whether the patient will benefit from PEG in the face of the potential decrease in quality of life.
The American Academy of Hospice and Palliative Medicine states that when a person approaches death, ANH is potentially harmful, may provide little or no benefit to the patient, and may make the period of dying more uncomfortable for both the patient and family. 154 In its position statement on ANH near the end of life, the Academy reports that metabolic function naturally declines at end of life and that the body cannot adequately utilize nutrition and hydration. Sampson et al 155 completed a Cochrane Review that found that enteral feeding in patients with advanced dementia was of no benefit. They reported that the assumption that a patient is dying from starvation is inaccurate; rather, the patient’s condition would be more correctly be described as dehydrated. Huffman and Dunn 156 report that the medical evidence is quite clear that dehydration in the end stage of a terminal illness is a very natural and compassionate way to die. They described several beneficial effects of dehydration, such as less fluid in the lungs and therefore less congestion, making breathing easier; less fluid in the throat and therefore less need for suctioning; less pressure around tumors and therefore less pain; and less urination and therefore less need for changing the bed and less risk of bedsores. They noted that there are burdens of hydration (e.g., dry mouth and thirst), but that they can be alleviated with good mouth care, ice chips, sips of water, and mouth moisturizers.
Cranford 157 described conditions when it is ethically appropriate to withhold fluids and nutrition: the person is terminally ill, is imminently dying, or is actively dying. Two distinct categories where it is appropriate to withhold ANH include those in which (1) the disease process is so overwhelming that death will occur within a relatively short time despite continued medical care. Limiting ANH becomes more of a medical decision than a moral decision. This corresponds with a loss of appetite as the patient approaches end of life. (2) The medical or disabling condition is severe or irreversible, and, although ANH may result in prolonged survival, there will be severe and lasting neurologic or medical impairment.
When either of the above occurs, the ethical obligation shifts from preservation of life to following the patient’s wishes or doing what is in the individual’s best interest.
In balancing factors that go into decisions about whether to proceed with ANH, it is important to be able to clearly articulate the positive and negative sequelae of alternative feeding methods. The potential burdens and benefits of ANH are summarized in ▶ Table 20.4. 143
Benefits | Burdens |
Aids in recovery from | Nausea, regurgitation, vomiting |
Acute events (e.g., stroke) | Respiratory congestion |
GI disorders/cancer | Diarrhea |
Allows for supplementation during chemotherapy/radiation therapy | Esophageal perforation |
Supplies nutrition for patients with neurogenic dysphagia without obstruction | Infection |
Aspiration of tube feeding | |
Local wound infections and painful insertion sites | |
Agitated behavior in individuals with cognitive impairments |
Plonk 158 offers the following guidelines for use of PEG tube in certain patient populations:
In early head and neck cancer patients, PEG can offset dysphagia and odynophagia during treatment and in the recuperative phase.
In 1999, the American Academy of Neurology developed evidence-based guidelines for the management of patients with ALS aimed at preservation of quality of life. In accordance with the guidelines, PEG should be considered before forced vital capacity falls below 50%. 159
PEG is useful in patients with malignant bowel obstructions with intractable vomiting.
PEG is appropriate for a patient with acute stroke and dysphagia persisting 1 month after hospital discharge.
The three most common reasons for tube feeding include (1) the patient’s inability to sustain nutrition orally, although the swallow response is safe; (2) the requirement for sufficient calories on a short-term basis; and (3) the risk of tracheal aspiration if the patient is allowed to eat orally. 160 Ideally, the SLP should be able to discuss various options for nonoral nutrition as well as the benefits and burdens of the commonly used options.
20.6.5 Team Approach
The medical team must come to a consensus regarding the patient’s prognosis for a reasonable degree of recovery in order to develop the appropriate plan of care, allowing the team to “speak with one voice.” 143 The authors provide the following guidelines for the swallow evaluation, which should include a review of the patient’s current and premorbid levels of function, medical status, nutrition and hydration status, and patient/family wishes. The question “How close is this patient to end of life?” must be answered. Brown’s End-of-Life Decision Tool ( ▶ Fig. 20.1) provides a visual means of determining how close a patient is to the end of life, weighing the patient’s premorbid level of function against their current medical status. Thus, a patient with a high level of function prior to the acute event who is medically stable has a reasonably good prognosis and will likely benefit from intervention, as opposed to one with a low premorbid level of function who is medically unstable or critically ill. Levy et al 143 propose that a “trial treatment period” may be indicated if the benefit from intervention is unclear.
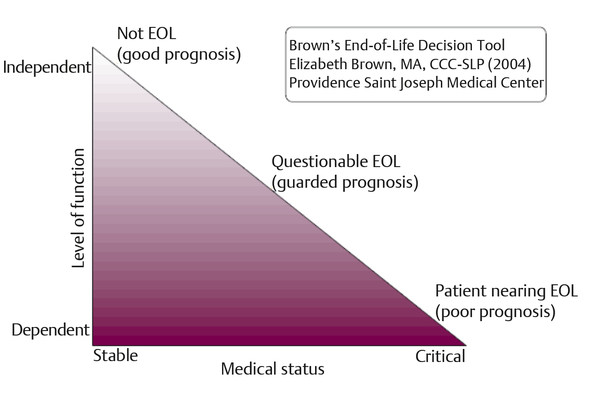
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


