Chronic Sclerosing Sialadenitis
Bruce M. Wenig, MD
Key Facts
Terminology
Chronic fibroinflammatory salivary gland disease with characteristic morphology that may represent IgG4-associated disease
Etiology/Pathogenesis
Increasing evidence that CSS, if IgG4 related, may be component of IgG4-related systemic disease
Prior to IgG4 association, sialolithiasis felt to be commonly associated with CSS of submandibular gland
May be true in percentage of non-IgG4-related cases
Clinical Issues
Primarily affects submandibular gland
IgG4-related sialadenitis steroid sensitive
Microscopic Pathology
Preservation of lobular architecture
Dense lymphoplasmacytic infiltrate within lobules
Large irregular lymphoid follicles with expanded geographic germinal centers
Sheets of mature plasma cells
Acinar atrophy
Lobules separated by fibrosis composed of fibroblasts and chronic inflammatory cells
Phlebitis (obliterative or nonobliterative) may or may not be identified
Ancillary Tests
Abundant IgG4(+) plasma cells present
IgG4(+) plasma cells present in inflamed lobules, interlobular septae, occasionally in germinal centers
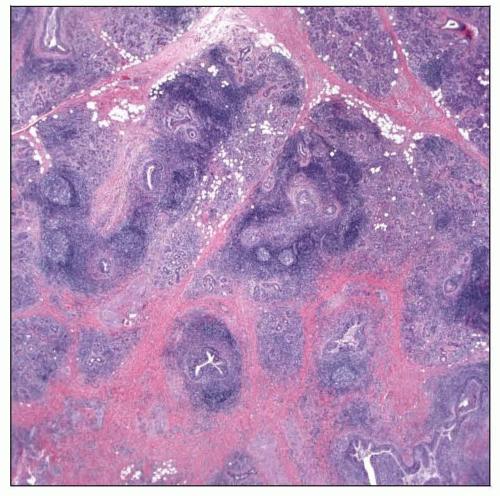 Submandibular chronic sclerosing sialadenitis is characterized by retention of the lobular architecture, dense inflammatory infiltrate, acinar atrophy, and interlobular fibrosis. |
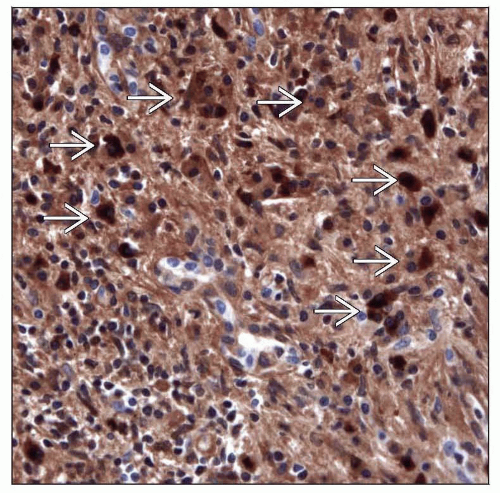 It is now recognized that submandibular chronic sclerosing sialadenitis may be an IgG4-related disease, confirmed by the presence of abundant IgG4 immunoreactive plasma cells  . . |
TERMINOLOGY
Abbreviations
Chronic sclerosing sialadenitis (CSS)
Synonyms
Küttner tumor
IgG4-associated sialadenitis
Punctate parotitis
Definitions
Chronic fibroinflammatory salivary gland disease with characteristic morphology that may represent IgG4- associated disease
ETIOLOGY/PATHOGENESIS
Immune-Mediated
Increasing evidence that CSS, if IgG4 related, may be component of IgG4-related systemic disease
IgG4-related diseases include
Autoimmune pancreatitis
Involvement of extrapancreatic organs including kidney, lung, retroperitoneum, liver, gallbladder, lymph nodes, breast, salivary glands, lacrimal gland, aorta
Morphologic features in CSS suggesting immune-mediated process include
Presence of prominent lymphoplasmacytic infiltrate and lymphoid follicles
Presence of unusual cytotoxic T-cell populations
Obstructive Sialadenitis
Prior to IgG4 association, sialolithiasis felt to be commonly associated with CSS of submandibular gland
May be true in percentage of non-IgG4-related cases
CLINICAL ISSUES
Epidemiology
Incidence
Unknown, but under recognized
Age
Most often occurs in 4th to 7th decades
Gender
Affects males slightly more often than females
Site
Primarily affects submandibular gland
Rarely, multiple salivary glands (major and minor) may be affected in single patient
Presentation
Pain and swelling of affected gland common
Often associated with ingestion of food
Patients may present with asymptomatic swelling of affected gland
May be localized to salivary gland involvement
May be associated with sclerosing lesions in extrasalivary gland tissues (systemic IgG4-related disease)
Laboratory Tests
Serum IgG4, IgG, IgG4/IgG ratio (normally 3-6%) typically elevated
Antibodies present in Sjögren syndrome including anti-SS-A, anti-SS-B not found in CSS
Absence of antineutrophilic antibodies (cytoplasmic and perinuclear)
Eosinophilia, hypergammaglobulinemia, and antinuclear antibodies (ANA) may be present in systemic but not localized disease
Treatment
Prognosis
IgG4-related
Excellent response to steroid
Sialolithiasis-related
Removal of stone results in reduction in swelling and pain
Rarely, extranodal marginal zone B-cell lymphoma (MALT) of salivary gland and salivary duct carcinoma may arise in background of CSS
IMAGE FINDINGS
Radiographic Findings
Sonographic findings usually show diffuse involvement of submandibular gland
Less often, focal involvement may occur
Diffuse involvement of gland may simulate sonographic appearance of “cirrhotic” liver
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


