12 CARDIOVASCULAR SYSTEM
General characteristics of the cardiovascular system
Arteries transport blood under high pressure and their muscular walls are thick (Figure 12-1). The veins are conduits for transport of the blood from tissues back to the heart. The pressure in the venous system is very low and the walls of the veins are thin.
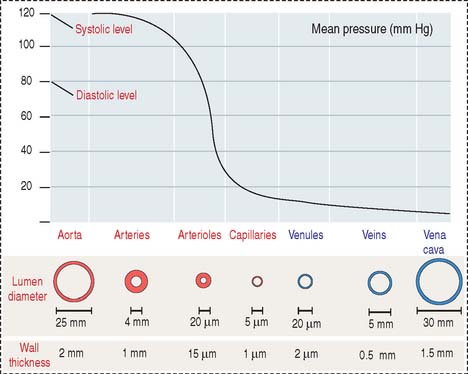
There are variations in blood pressure in various parts of the cardiovascular system (see Figure 12-1). Because the heart pumps blood continuously in a pulsatile fashion into the aorta, the pressure in the aorta is high (about 100 mm Hg) and the arterial pressure fluctuates between a systolic level of 120 mm Hg and a diastolic level of 80 mm Hg.
HEART
The heart is a folded endothelial tube whose wall is thickened to act as a regulated pump. The heart is the major determinant of systemic blood pressure.
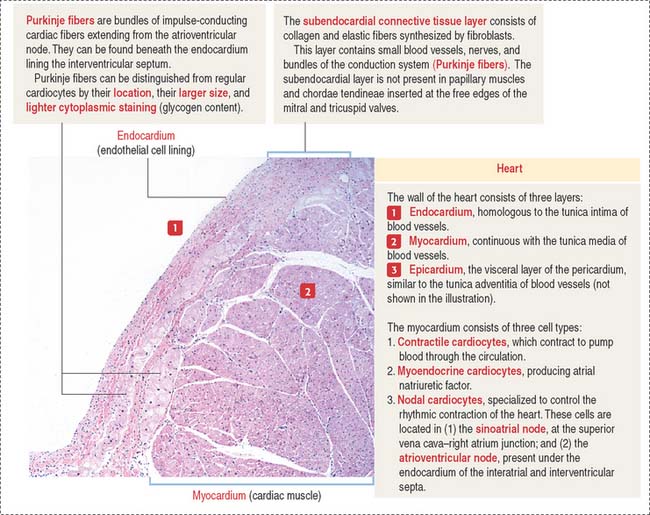
The cardiac wall consists of three layers:
Conductive system of the heart
The heart has two specialized conductive systems:
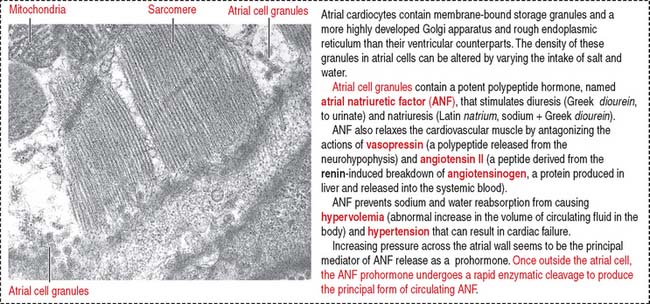
When stretched, cardiac muscle cells of the atrium (atrial cardiocytes) secrete a peptide called atrial natriuretic factor (ANF) (Figure 12-3) that stimulates both diuresis and excretion of sodium in urine (natriuresis) by increasing the glomerular filtration rate. By this mechanism, the blood volume is reduced.
Histologically (see Figure 7-18 in Chapter 7, Muscle Tissue), individual cardiac muscle cells have a central nucleus and are linked to each other by intercalated disks. The presence of gap junctions in the longitudinal segment of the intercalated disks between connected cardiac muscle cells allows free diffusion of ions and the rapid spread of the action potential from cell to cell. The electrical resistance is low because gap junctions bypass the transverse components of the intercalated disk (fasciae adherentes and desmosomes).
Differences between cardiac muscle fibers and Purkinje fibers
The Purkinje fibers lie beneath the endocardium lining the two sides of the interventricular septum (see Figure 12-2). They can be distinguished from cardiac muscle fibers because they contain a reduced number of myofibrils located at the periphery of the fiber and the diameter of the fiber is larger. In addition, they give a positive reaction for acetylcholinesterase, and they contain abundant glycogen. Purkinje fibers lose these specific characteristics when they merge with cardiac muscle fibers. Like cardiac muscle fibers, Purkinje fibers are striated and are linked to each other by atypical intercalated disks.
ARTERIES
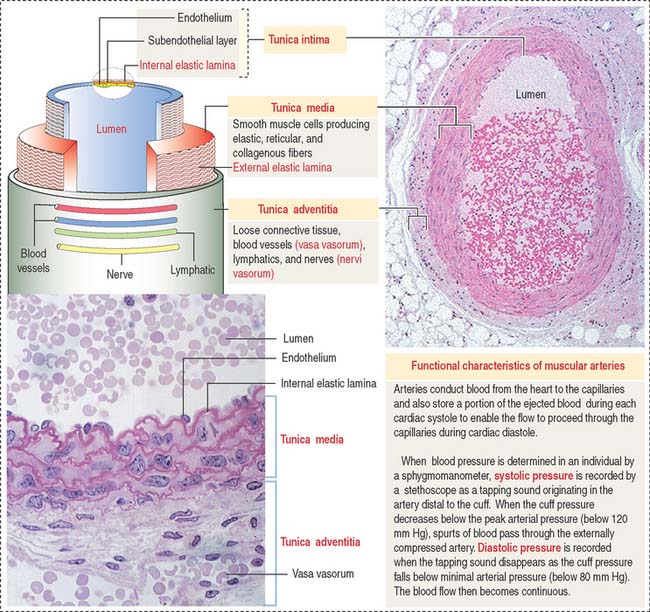
Arteries are organized in three major tunics or layers (Figure 12-4):
From the heart to the capillaries, arteries can be classified into three major groups: (1) large elastic arteries, (2) medium-sized muscular arteries (see Figure 12-4), and (3) small arteries and arterioles.
Large elastic arteries are conducting vessels
The aorta and its largest branches (the brachiocephalic, common carotid, subclavian, and common iliac arteries) are elastic arteries (Figure 12-5). They are conducting arteries because they conduct blood from the heart to the medium-sized distributing arteries.
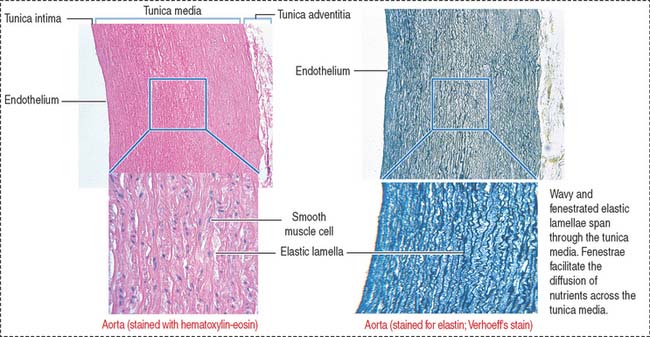
Large amounts of fenestrated elastic sheaths are found in the tunica media, with bundles of smooth muscle cells permeating the narrow gaps between the elastic lamellae. Collagen fibers are present in all tunics, but especially in the adventitia. We have seen in Chapter 4, Connective Tissue, that smooth muscle cells can synthesize both elastic and collagen fibers. Blood vessels (vasa vasorum), nerves (nervi vasorum), and lymphatics can be recognized in the tunica adventitia of large elastic arteries.
Clinical significance: Aortic aneurysms
The two major types of aortic aneurysms are the syphilitic aneurysm (relatively rare because syphilis is no longer common) and the abdominal aneurysm. The latter is caused by a weakening of the aortic wall produced by atherosclerosis (see Figure 12-14). Aortic aneurysms generate murmurs caused by blood turbulence in the dilated aortic segment. A severe complication is rupture of the aneurysm followed by immediate death.
Marfan syndrome (see Chapter 4, Connective Tissue) is an autosomal dominant defect associated with aortic dissecting aneurysm and skeletal and ocular abnormalities due to mutations in the fibrillin 1 gene. Fibrillins are major components of the elastic fibers found in the aorta, periosteum, and suspensory ligament of the lens.
Medium-sized muscular arteries are distributing vessels
There is a gradual transition from large arteries, to medium-sized arteries, to small arteries and arterioles. Medium-sized arteries are distributing vessels, allowing a selective distribution of blood to different organs in response to functional needs. Examples of medium-sized arteries include the radial, tibial, popliteal, axillary, splenic, mesenteric, and intercostal arteries. The diameter of medium-sized muscular arteries is about 3 mm or greater.
The tunica intima consists of three layers: (1) the endothelium, (2) the sub-endothelium, and (3) the internal elastic lamina (see Figure 12-4).
Arterioles are resistance vessels
Arterioles are the final branches of the arterial system. Arterioles regulate the distribution of blood to different capillary beds by vasoconstriction and vasodilation in localized regions. Partial contraction (known as tone) of the vascular smooth muscle exists in arterioles. Arterioles are structurally adapted for vasoconstriction and vasodilation because their walls contain circularly arranged smooth muscle fibers. Arterioles are regarded as resistance vessels and are the major determinants of systemic blood pressure (Figure 12-6).
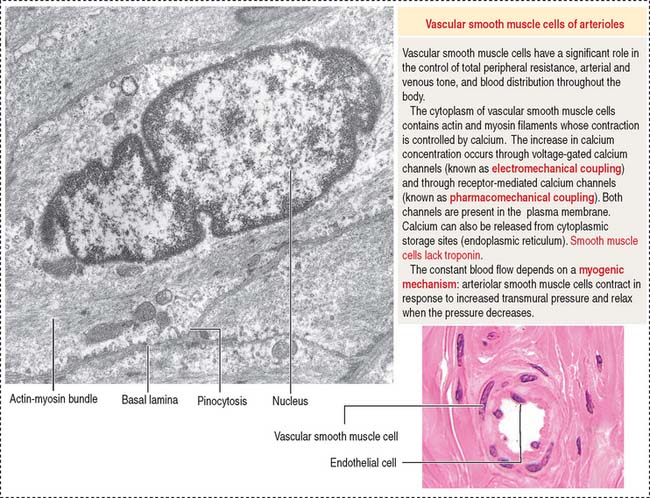
The diameter of arterioles and small arteries ranges from 20 to 130 μm. Because the lumen is small, these blood vessels can be closed down to generate high resistance to blood flow. The tunica intima has an endothelium, subendothelium, and internal elastic lamina. The tunica media consists of two to five concentric layers of smooth muscle cells. The tunica adventitia, or tunica externa, contains slight collagenous tissue, binding the vessel to its surroundings.
Capillaries are exchange vessels
The microvascular bed, the site of the microcirculation (Figure 12-7), is composed of the terminal arteriole (and metarteriole), the capillary bed, and the postcapillary venules. The capillary bed consists of slightly large capillaries (called preferential or thoroughfare channels), where blood flow is continuous, and small capillaries, called the true capillaries, where blood flow is intermittent.
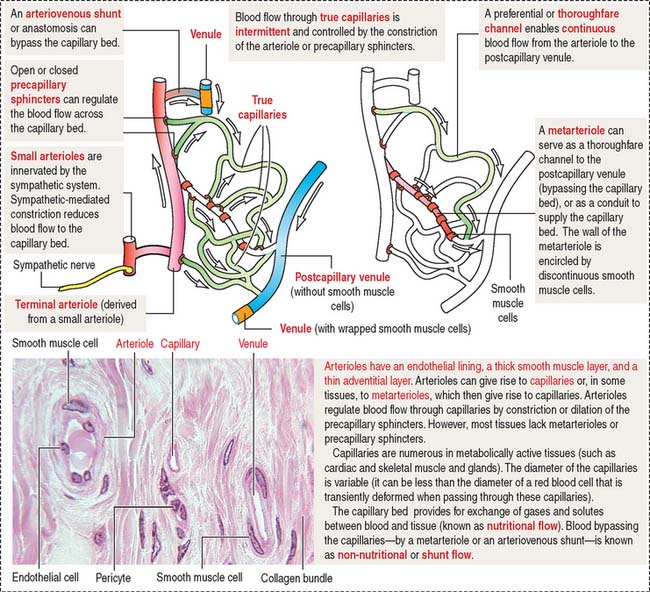
When functional demands decrease, most precapillary sphincters are closed, forcing the flow of blood into thoroughfare channels. Arteriovenous shunts, or anastomoses, are direct connections between arterioles and postcapillary venules and bypass the microvascular bed.
Three types of capillaries: Continuous, fenestrated, and discontinuous
Three morphologic types of capillaries are recognized (Figures 12-8 and 12-9): continuous, fenestrated, and discontinuous (sinusoids).
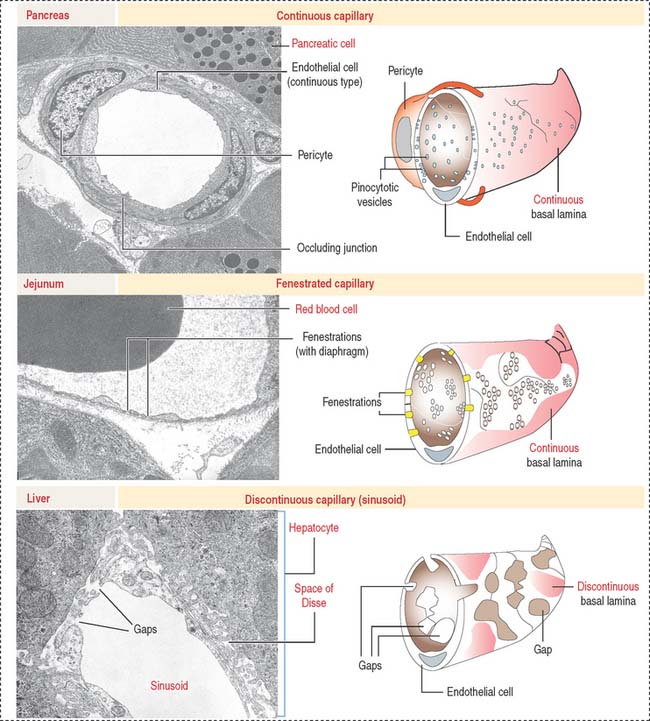
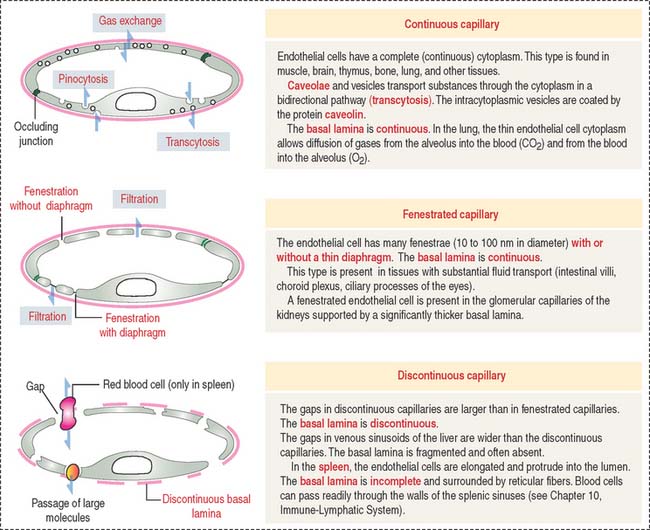
Fenestrated capillaries have pores, or fenestrae, with or without diaphragms. Fenestrated capillaries with a diaphragm are found in intestines, endocrine glands, and around kidney tubules. Fenestrated capillaries without a diaphragm are characteristic of the renal glomerulus. In this particular case, the basal lamina constitutes an important permeability barrier, as we will analyze in Chapter 14, Urinary System.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


