Chapter 11 Cardiology
Angiotensin-Converting Enzyme Inhibitors (ACEIs)


MOA (Mechanism of Action)



 Through inhibition of ACE with an ACEI, the following effects occur:
Through inhibition of ACE with an ACEI, the following effects occur: Net result: Because angiotensin II levels are lower and bradykinin levels are higher, there is more vasodilation; SVR (systemic vascular resistance) and afterload are lowered. Because aldosterone levels are lower, less Na and water are reabsorbed in the kidney; therefore preload is reduced (Figure 11-1).
Net result: Because angiotensin II levels are lower and bradykinin levels are higher, there is more vasodilation; SVR (systemic vascular resistance) and afterload are lowered. Because aldosterone levels are lower, less Na and water are reabsorbed in the kidney; therefore preload is reduced (Figure 11-1).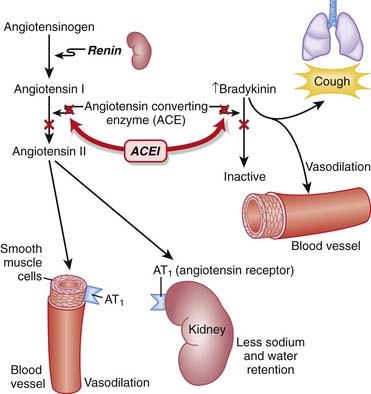
Pharmacokinetics
 Most ACEIs are cleared predominantly by the kidneys. Dose adjustment should be considered in renal impairment.
Most ACEIs are cleared predominantly by the kidneys. Dose adjustment should be considered in renal impairment.



Contraindications
 Pregnancy: During the second and third trimesters, the teratogenic effects are thought to be caused in part by fetal hypotension.
Pregnancy: During the second and third trimesters, the teratogenic effects are thought to be caused in part by fetal hypotension.
Side Effects
 Dry cough: Attributed to increased bradykinin levels. Can be persistent enough to affect compliance and may lead to discontinuation.
Dry cough: Attributed to increased bradykinin levels. Can be persistent enough to affect compliance and may lead to discontinuation.



Important Notes
 The renin-angiotensin system (RAS) plays an important role in the body’s compensation for a failing heart. Activation of the sympathetic nervous system (SNS) leads to the release of renin, which in turn increases vascular tone and sodium and water retention.
The renin-angiotensin system (RAS) plays an important role in the body’s compensation for a failing heart. Activation of the sympathetic nervous system (SNS) leads to the release of renin, which in turn increases vascular tone and sodium and water retention.
Advanced
 In addition to the beneficial effects of RAS inhibitors in diabetic nephropathy, there is emerging evidence that RAS inhibitors may reduce the incidence of new-onset diabetes. Potential mechanisms for this effect include improvements in blood flow that improve the delivery of insulin and glucose to skeletal muscle, as well as effects on glucose transport and insulin signaling. If this preventative effect of RAS inhibition in diabetes becomes established, it could change the way these agents are used.
In addition to the beneficial effects of RAS inhibitors in diabetic nephropathy, there is emerging evidence that RAS inhibitors may reduce the incidence of new-onset diabetes. Potential mechanisms for this effect include improvements in blood flow that improve the delivery of insulin and glucose to skeletal muscle, as well as effects on glucose transport and insulin signaling. If this preventative effect of RAS inhibition in diabetes becomes established, it could change the way these agents are used.
Evidence
Hypertension
 A 2009 Cochrane review (24 trials, N = 58,040 participants) compared benefits and harms of first-line antihypertensives with those of placebo or no treatment over a minimum of 1 year in patients with hypertension. ACEIs (three trials) reduced mortality (relative risk [RR] 0.83), stroke (RR 0.65), coronary heart disease (RR 0.81), and cardiovascular events (RR 0.76).
A 2009 Cochrane review (24 trials, N = 58,040 participants) compared benefits and harms of first-line antihypertensives with those of placebo or no treatment over a minimum of 1 year in patients with hypertension. ACEIs (three trials) reduced mortality (relative risk [RR] 0.83), stroke (RR 0.65), coronary heart disease (RR 0.81), and cardiovascular events (RR 0.76).



Angiotensin Receptor Blockers (ARBs)


MOA (Mechanism of Action)
 ARBs are antagonists of the angiotensin-1 (AT1) receptor. Therefore they block the actions of angiotensin II.
ARBs are antagonists of the angiotensin-1 (AT1) receptor. Therefore they block the actions of angiotensin II.



 Conversely, ACE is not the only enzyme that forms angiotensin II. Thus ARBs might provide more complete inhibition of the vasopressor activity of angiotensin II compared with ACEIs (Figure 11-2).
Conversely, ACE is not the only enzyme that forms angiotensin II. Thus ARBs might provide more complete inhibition of the vasopressor activity of angiotensin II compared with ACEIs (Figure 11-2).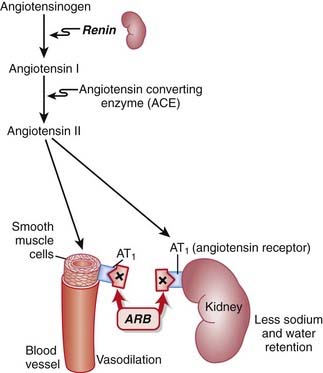
Pharmacokinetics
 All ARBs have intermediate (12 to 24 hour) half-lives and thus provide the advantage of once-daily dosing.
All ARBs have intermediate (12 to 24 hour) half-lives and thus provide the advantage of once-daily dosing.









Important Notes
 Perhaps because of the lack of increased bradykinin levels, ARBs are not typically associated with the side effect of cough, which can be a significant limitation to the use of ACEIs.
Perhaps because of the lack of increased bradykinin levels, ARBs are not typically associated with the side effect of cough, which can be a significant limitation to the use of ACEIs.
Advanced
 In addition to the beneficial effects of RAS inhibitors in diabetic nephropathy, there is emerging evidence that RAS inhibitors may reduce the incidence of new-onset diabetes. Potential mechanisms for this effect include improvements in blood flow that improve the delivery of insulin and glucose to skeletal muscle, as well as effects on glucose transport and insulin signaling. If this preventative effect of RAS inhibition in diabetes becomes established, it could change the way these agents are used.
In addition to the beneficial effects of RAS inhibitors in diabetic nephropathy, there is emerging evidence that RAS inhibitors may reduce the incidence of new-onset diabetes. Potential mechanisms for this effect include improvements in blood flow that improve the delivery of insulin and glucose to skeletal muscle, as well as effects on glucose transport and insulin signaling. If this preventative effect of RAS inhibition in diabetes becomes established, it could change the way these agents are used.





Direct Renin Inhibitors

MOA (Mechanism of Action)
 Renin is an enzyme released from the kidneys that converts angiotensinogen to angiotensin I. It is considered to be the rate-limiting step in the eventual formation of angiotensin II.
Renin is an enzyme released from the kidneys that converts angiotensinogen to angiotensin I. It is considered to be the rate-limiting step in the eventual formation of angiotensin II.








 Therefore, one potential advantage of renin antagonists over ACEIs and ARBs is avoiding the compensatory increase in the RAS. It is yet to be established whether these theoretical advantages translate into clinically meaningful advantages (Figure 11-3).
Therefore, one potential advantage of renin antagonists over ACEIs and ARBs is avoiding the compensatory increase in the RAS. It is yet to be established whether these theoretical advantages translate into clinically meaningful advantages (Figure 11-3).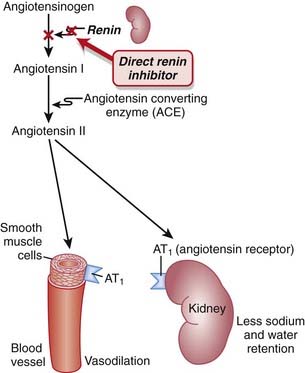











Evidence
Blood-Pressure Lowering Efficacy versus Placebo
 A 2008 Cochrane review (six trials, 3694 participants) compared the blood-pressure–lowering efficacy of renin inhibitors versus placebo in primary HTN. The authors found that aliskiren elicits a dose-dependent reduction in both systolic and diastolic pressure similar to that seen with ACEIs or ARBs. In the included trials, aliskiren did not increase withdrawals due to adverse events versus placebo.
A 2008 Cochrane review (six trials, 3694 participants) compared the blood-pressure–lowering efficacy of renin inhibitors versus placebo in primary HTN. The authors found that aliskiren elicits a dose-dependent reduction in both systolic and diastolic pressure similar to that seen with ACEIs or ARBs. In the included trials, aliskiren did not increase withdrawals due to adverse events versus placebo.FYI Notes
 Renin was first identified in 1898, when it was extracted from kidneys and discovered to have pressor properties. It would be another 40 years before it was determined that renin was an enzyme that catalyzed the formation of a pressor substance (angiotensin II), rather than being the pressor itself.
Renin was first identified in 1898, when it was extracted from kidneys and discovered to have pressor properties. It would be another 40 years before it was determined that renin was an enzyme that catalyzed the formation of a pressor substance (angiotensin II), rather than being the pressor itself.

Sodium Channel Blockers (Class I Antiarrhythmics)
Description
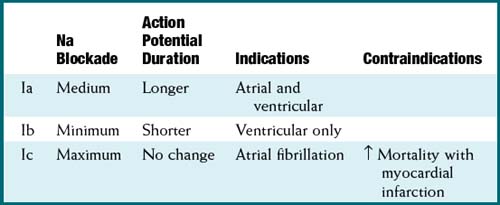
Na channel blockers are Vaughan Williams class I antiarrhythmics. There are three subclasses: Ia, Ib, and Ic. The use of Na channel blockers as local anesthetics is discussed in the discussion of local anesthetics in Chapter 21.



MOA (Mechanism of Action)
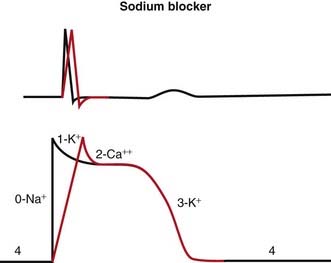
 Na channels are blocked, so Na ion movement during phase 0 of the action potential is inhibited. The result is a “slow” phase 0, which results in a wider (and slower) QRS wave on the electrocardiogram (ECG). The net result is slower conduction (Figure 11-4).
Na channels are blocked, so Na ion movement during phase 0 of the action potential is inhibited. The result is a “slow” phase 0, which results in a wider (and slower) QRS wave on the electrocardiogram (ECG). The net result is slower conduction (Figure 11-4).













Pharmacokinetics
 Quinidine interacts with digoxin (CP450). This can result in increased levels of digoxin, a toxic drug with a narrow therapeutic index. Both drugs are antiarrhythmic drugs and have the potential to be coadministered.
Quinidine interacts with digoxin (CP450). This can result in increased levels of digoxin, a toxic drug with a narrow therapeutic index. Both drugs are antiarrhythmic drugs and have the potential to be coadministered.

Side Effects
 Proarrhythmic: As with all antiarrhythmics, changing the delicate balance of conduction speed and refractory times might provoke another area of the conducting system into developing a dysrhythmia.
Proarrhythmic: As with all antiarrhythmics, changing the delicate balance of conduction speed and refractory times might provoke another area of the conducting system into developing a dysrhythmia.


Evidence
 Atrial fibrillation and prevention of recurrence: A Cochrane review in 2007 (45 studies, 12,559 patients) evaluated the efficacy and safety of multiple different antiarrhythmics in patients who had previously experienced atrial fibrillation (a very common arrhythmia). Class Ia antiarrhythmics were associated with increased mortality compared with controls (odds ratio [OR] 2.39; number needed to harm [NNH] 109). Class Ia and Ic were associated with reduced occurrences of atrial fibrillation (OR 0.19 to 0.6). There were many withdrawals from treatment because of side effects for all antiarrhythmics (NNH 17 to 36).
Atrial fibrillation and prevention of recurrence: A Cochrane review in 2007 (45 studies, 12,559 patients) evaluated the efficacy and safety of multiple different antiarrhythmics in patients who had previously experienced atrial fibrillation (a very common arrhythmia). Class Ia antiarrhythmics were associated with increased mortality compared with controls (odds ratio [OR] 2.39; number needed to harm [NNH] 109). Class Ia and Ic were associated with reduced occurrences of atrial fibrillation (OR 0.19 to 0.6). There were many withdrawals from treatment because of side effects for all antiarrhythmics (NNH 17 to 36).

β Antagonists (β-Blockers)
Prototype and Common Drugs







MOA (Mechanism of Action)
To understand β-blockers, you must understand the effects of the adrenergic system and which effects are mediated via β receptors. β-Blockers competitively antagonize the action of catecholamines at β receptors. There are many cardiac and noncardiac consequences of β-blockade. More details on the autonomic nervous system are described in Chapter 3.







Tachycardia and Arrhythmia
The properties of β-blockers that make them antitachycardics include the following:
1 Depression of the sinoatrial (SA) node (slows automaticity)
 Catecholamine β1 stimulation results in an increase in the slow Na+ current (If) of the action potential phase 4 in the SA node. This results in a faster rising (and shorter) phase 4, a shorter time to the next heartbeat, and thus a faster HR. β-Blockers will oppose this action, slowing the SA pacemaker rate.
Catecholamine β1 stimulation results in an increase in the slow Na+ current (If) of the action potential phase 4 in the SA node. This results in a faster rising (and shorter) phase 4, a shorter time to the next heartbeat, and thus a faster HR. β-Blockers will oppose this action, slowing the SA pacemaker rate.
Catecholamine β1 stimulation results in an increase in the slow Na+ current (If) of the action potential phase 4 in the SA node. This results in a faster rising (and shorter) phase 4, a shorter time to the next heartbeat, and thus a faster HR. β-Blockers will oppose this action, slowing the SA pacemaker rate.
2 Depression of the AV node (prolongs the refractory period)
 Same mechanism as SA node: a decrease in the slow Na+ current (If) leaves the AV node in a refractory state longer.
Same mechanism as SA node: a decrease in the slow Na+ current (If) leaves the AV node in a refractory state longer.
Same mechanism as SA node: a decrease in the slow Na+ current (If) leaves the AV node in a refractory state longer.








Myocardial Ischemia and Infarction








Pharmacokinetics
 Shorter half-lives (3 to 4 hours): propranolol, metoprolol (sustained-release forms with longer half-lives are available)
Shorter half-lives (3 to 4 hours): propranolol, metoprolol (sustained-release forms with longer half-lives are available)












Contraindications
 Asthmatics should not use nonselective (β1, β2) β-blockers, as blocking β2 receptors may lead to bronchoconstriction. Stimulation of β2 receptors in the airways causes smooth muscle relaxation of the bronchioles and is the basis of bronchodilators that are β2 agonists.
Asthmatics should not use nonselective (β1, β2) β-blockers, as blocking β2 receptors may lead to bronchoconstriction. Stimulation of β2 receptors in the airways causes smooth muscle relaxation of the bronchioles and is the basis of bronchodilators that are β2 agonists.













Important Notes
 β-blockers should not be discontinued abruptly, because of a rebound effect that might result in tachycardia and exacerbate the symptoms of coronary artery disease or might induce a hypertensive effect. The rebound appears to be an overactivity of the SNS, caused perhaps by receptor up-regulation.
β-blockers should not be discontinued abruptly, because of a rebound effect that might result in tachycardia and exacerbate the symptoms of coronary artery disease or might induce a hypertensive effect. The rebound appears to be an overactivity of the SNS, caused perhaps by receptor up-regulation.



Evidence

After Myocardial Infarction
 Evidence for the role of β-blockers in secondary prevention after an MI comes from several trials and was summarized in a 1999 systematic review (82 trials, N = 54,234 patients). There was a 23% reduction in the odds of death in long-term trials but only a 4% reduction in short-term trials. The review found that the number needed to treat (NNT) to avoid a fatality over the course of 2 years is 42. The greatest amount of evidence available was for propranolol, timolol, and metoprolol.
Evidence for the role of β-blockers in secondary prevention after an MI comes from several trials and was summarized in a 1999 systematic review (82 trials, N = 54,234 patients). There was a 23% reduction in the odds of death in long-term trials but only a 4% reduction in short-term trials. The review found that the number needed to treat (NNT) to avoid a fatality over the course of 2 years is 42. The greatest amount of evidence available was for propranolol, timolol, and metoprolol.Hypertension and Associated Stroke and Coronary Artery Disease
 A Cochrane review in 2007 (13 studies, N = 91,561 patients) compared β-blockers with other agents for HTN. Atenolol was the β-blocker most frequently used. The authors found that β-blockers had only weak effects in reducing stroke and no effect on coronary heart disease versus placebo. There was also a trend toward worse outcomes when compared with calcium channel blockers (CCBs), RAS inhibitors, and thiazides, prompting the authors to suggest that β-blockers should not be considered as first-line agents for HTN.
A Cochrane review in 2007 (13 studies, N = 91,561 patients) compared β-blockers with other agents for HTN. Atenolol was the β-blocker most frequently used. The authors found that β-blockers had only weak effects in reducing stroke and no effect on coronary heart disease versus placebo. There was also a trend toward worse outcomes when compared with calcium channel blockers (CCBs), RAS inhibitors, and thiazides, prompting the authors to suggest that β-blockers should not be considered as first-line agents for HTN.Obstructive Airway Disease (Asthma and Chronic Obstructive Pulmonary Disease)
 A Cochrane review in 2002 (29 studies, N = 381 patients) examined the impact of single-dose or short-term selective β1-blockers in patients with mild to moderate obstructive airway disease. There were no differences in pulmonary flow measurements compared with placebo except for a small decrease in FEV1 after the first treatment—an effect that disappeared with subsequent doses.
A Cochrane review in 2002 (29 studies, N = 381 patients) examined the impact of single-dose or short-term selective β1-blockers in patients with mild to moderate obstructive airway disease. There were no differences in pulmonary flow measurements compared with placebo except for a small decrease in FEV1 after the first treatment—an effect that disappeared with subsequent doses.

Potassium Channel Blockers (Class III Antiarrhythmics)





MOA (Mechanism of Action)
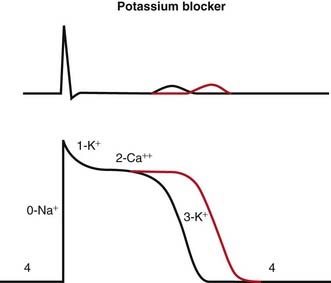
 Blocking K channels in phase 3 of the action potential slows the efflux of K back out of the myocyte, which slows the rate at which the cell repolarizes and therefore lengthens the plateau phase of the action potential. This increases the refractory period of atrial, ventricular, and Purkinje cells. This also increases the QT interval on the ECG (Figure 11-5).
Blocking K channels in phase 3 of the action potential slows the efflux of K back out of the myocyte, which slows the rate at which the cell repolarizes and therefore lengthens the plateau phase of the action potential. This increases the refractory period of atrial, ventricular, and Purkinje cells. This also increases the QT interval on the ECG (Figure 11-5).
Pharmacokinetics

 Drug interactions:
Drug interactions: Amiodarone and dronedarone are metabolized by and are inhibitors of CYP3A4; this is important because other drugs used in the control of dysrhythmias, including verapamil and diltiazem, are also metabolized by CYP3A4, and drug levels can be increased when drugs are coadministered.
Amiodarone and dronedarone are metabolized by and are inhibitors of CYP3A4; this is important because other drugs used in the control of dysrhythmias, including verapamil and diltiazem, are also metabolized by CYP3A4, and drug levels can be increased when drugs are coadministered.





