Carcinoid
Joel K. Greenson, MD
Key Facts
Clinical Issues
Carcinoid syndrome (< 10% of patients)
Most often asymptomatic incidental finding
2/3 of patients with carcinoid syndrome get fibrous endocardial thickening of right heart
Somatostatin analogs (octreotide and lanreotide) can successfully treat symptoms and even shrink tumors
Depends on stage and grade of tumor (WHO classification)
Small bowel carcinoids have worse prognosis than those in stomach or rectum
Image Findings
Octreoscan: Highly sensitive test using radiolabeled somatostatin analog to localize tumors
Microscopic Pathology
Nested or trabecular pattern of fairly homogeneous (and often bland) cells
Very vascular tumor
Well-differentiated tumors have few mitoses and bland nuclei (“salt & pepper” chromatin)
Poorly differentiated tumors have high mitotic rate (Ki-67 > 30%), necrosis
Angiolymphatic invasion frequently seen even in low-grade lesions
Ancillary Tests
CD56 best marker for small cell carcinoma
Top Differential Diagnoses
Lymphoma
Adenocarcinoma
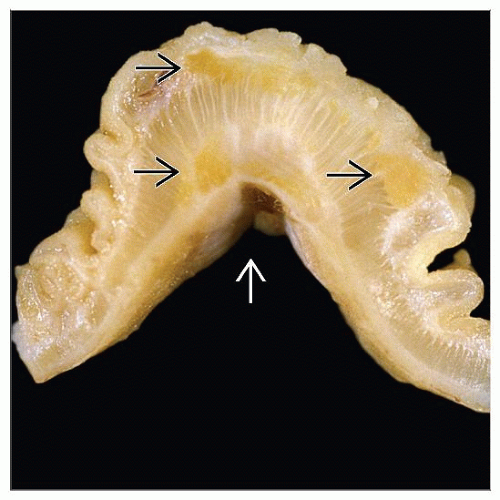 Gross pathology photograph shows a submucosal tumor that has caused a kink in the bowel wall  . Nests of tumor cells can be seen as yellow areas . Nests of tumor cells can be seen as yellow areas  that infiltrate the bowel wall. that infiltrate the bowel wall. |
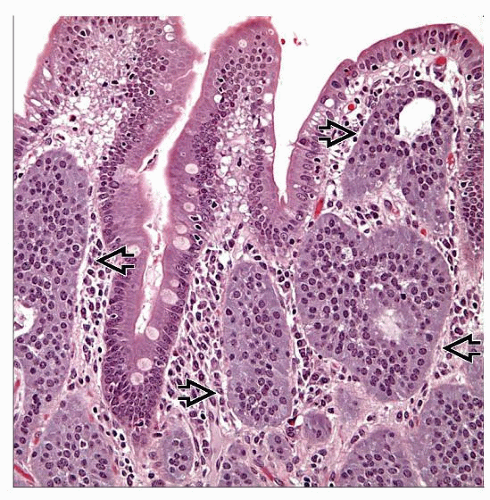 Hematoxylin & eosin shows multiple nests of well-differentiated neuroendocrine tumors  within the mucosa. within the mucosa. |
TERMINOLOGY
Synonyms
Well-differentiated neuroendocrine tumor (carcinoid)
Well-differentiated neuroendocrine carcinoma (malignant carcinoid)
Definitions
Neoplasm composed primarily of cells with neuroendocrine differentiation
CLINICAL ISSUES
Epidemiology
Incidence
Approximately 2/100,000 in USA and Europe
Incidence increasing over time, perhaps due to better detection methods
Age
Incidence increases with age, much more common in patients > 50
Gender
Small bowel carcinoids more common in men
Gastric carcinoids more common in women
Ethnicity
More common in African-Americans (almost 2x prevalence seen in Caucasians)
Site
Duodenum: 5 types of tumors
Gastrinomas
May be sporadic but often associated with MEN1 and Zollinger-Ellison syndrome
Typically small but often have large lymph node metastases
Somatostatinomas
Occur in and around ampulla
Glandular architecture with psammoma bodies
Associated with neurofibromatosis type 1 and MEN1
15% of duodenal endocrine tumors
Nonfunctioning tumors
Better prognosis
Poorly differentiated neuroendocrine carcinomas
Undifferentiated or small cell: Very aggressive
Hormonally inactive
Will stain with synaptophysin but little or no positivity with chromogranin-A
Gangliocytic paraganglioma
Excellent prognosis
Jejunum and ileum
More likely to have metastatic disease at time of presentation (64%)
Multicentric in ˜ 30% of cases
5 year survival of 60%
Presentation
Abdominal pain
Carcinoid syndrome (< 10% of patients)
Diarrhea
Flushing
May also have bronchospasm, myopathy, arthropathy, and scleroderma of skin
2/3 of patients with carcinoid syndrome get fibrous endocardial thickening of right heart
May lead to tricuspid regurgitation and heart failure
Causes 1/3 of deaths from carcinoid syndrome
Painful mass
Obstructive symptoms
Most often asymptomatic incidental finding
Endoscopic Findings
Submucosal mass or nodule (smooth surface)
Laboratory Tests
Elevated levels of 5-HIAA in 24-hour urine collection
Elevated level of chromogranin-A in blood
Treatment
Surgical approaches
Surgical excision of primary lesions often necessary to prevent obstruction
Resection (debulking) of metastatic disease may relieve carcinoid syndrome symptoms but often only temporarily
Drugs
Somatostatin analogues (octreotide and lanreotide) can successfully treat symptoms and even shrink tumors
Chemotherapy and radiation therapy have very little effect on low-grade lesions
Prognosis
Depends on stage and grade of tumor (WHO classification)
Well-differentiated neuroendocrine tumor of duodenum and upper jejunum (benign) (carcinoid)
≤ 1 cm, no angiolymphatic invasion, confined to mucosa-submucosa
Well-differentiated neuroendocrine tumor of duodenum and upper jejunum (uncertain malignant potential)
1-2 cm, confined to mucosa-submucosa, ± angiolymphatic invasion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


