Carcinoid Tumor, Stomach
Gregory Y. Lauwers, MD
Key Facts
Clinical Issues
Gastric carcinoids represent 5% of all gastrointestinal carcinoids
Most carcinoids (type 1, 2, and 4) are fundic
Type 3 can arise anywhere in gastric mucosa
Majority of gastric carcinoids are slowly growing, locally infiltrative, and generally of low-grade malignancy
Endoscopic resection advocated for small tumors limited in numbers
Antrectomy that removes hypergastrinemic drive advocated for type 1 carcinoid
Metastases do not preclude long-term survival
Macroscopic Features
Commonly multiple
Small, smooth, firm, circumscribed, polypoid elevations of mucosa and submucosa
Microscopic Pathology
Small cuboidal cells with round nuclei with evenly dispersed chromatin
Solid, trabecular, and ribbon-like arrangement
Commonly infiltrate submucosa but seldom deeper
High-grade sporadic carcinoid tumor may resemble small cell carcinoma
Immunocytochemistry positive for chromogranin-A, synaptophysin, Leu-7 and PGP9.5, and CEA-M
Background corpus mucosa of type 1, 2, and 4 carcinoids shows various patterns of ECL-cell hyperplasia
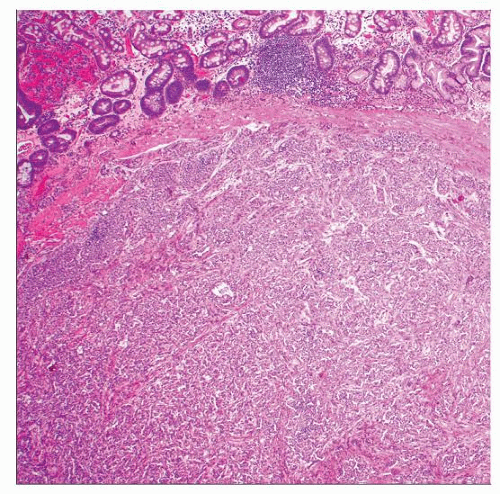 Hematoxylin & eosin shows a distinct invasive carcinoid extending the submucosa. Even at this low power, the insular and trabecular organization can be recognized. |
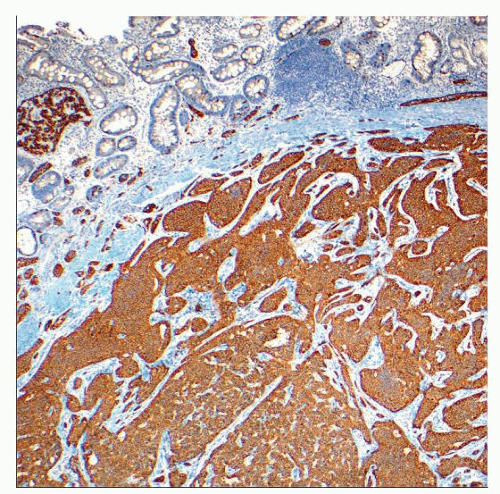 Synaptophysin of the corresponding case confirms the histologic diagnosis and highlights the architecture of the tumor. |
TERMINOLOGY
Definitions
Neuroendocrine neoplasms arising from enterochromaffin-like (ECL) cells
> 0.5 mm in size or invading submucosa
ETIOLOGY/PATHOGENESIS
Autoimmune Gastritis
Related to type 1 carcinoid (75% of cases)
Gastrin hypersecretion causes hyperplasia and neoplastic transformation of gastric ECL cells
Zollinger-Ellison Syndrome Associated with MEN1
Related to type 2 carcinoid (5-10% of cases)
Gastrin hypersecretion by gastrin-secreting tumor causes hyperplasia and neoplastic transformation of gastric ECL cells
Sporadic
Related to solitary and larger type 3 carcinoids
Defect of Acid Secretion by Parietal Cells
Related to type 4 carcinoids
Hypergastrinemia is secondary to achlorhydria
CLINICAL ISSUES
Epidemiology
Incidence
5% of all gastrointestinal carcinoids
1% of all gastric tumors
Age
Middle-aged adults
Gender
Type 1 and 2 tumors more common in women
Men overrepresented in type 3 tumors
Site
Most carcinoids (type 1, 2, and 4) are fundic
Type 3 carcinoids can arise anywhere in gastric mucosa
Presentation
50% of patients with type 1 carcinoids have pernicious anemia
Patients with type 2 carcinoids will present with symptoms of Zollinger-Ellison and MEN1
Sporadic type 3 tumors are larger and may produce symptoms suggestive of gastric carcinoma
Hemorrhage, obstruction, or metastasis
Peptide hormone hypersecretion-related symptoms are uncommon
Atypical carcinoid syndrome has been reported
Cushing syndrome from ectopic corticotrophin secretion has been reported
Endoscopic Findings
Type 1, 2, and 4 carcinoids present as polypoid, yellowish nodules
Central erythematous depression
Multiple and limited to gastric corpus
Sporadic carcinoids tend to be solitary and larger
Natural History
Majority of gastric carcinoids are generally of low-grade malignancy
Slow growing and locally infiltrative
Tumors < 1 cm in diameter and confined to mucosa and submucosa rarely metastasize
Multiple type 1, 2, and 4 carcinoids are usually small (< 1 cm)
Type 1 carcinoids can regress with time
Large (usually type 3) tumors with vascular or muscularis propria invasion can spread to lymph nodes and liver
Rare functioning tumors that lead to clinical hypersecretion syndrome are always malignant
Treatment
Local excision or endoscopic resection
Advocated for small tumors up to 5 in number
Extirpation of new lesions as they arise
Antrectomy
Removal of antral G cells (which provide hypergastrinemic drive) advocated for type 1 carcinoid
Numerous or large carcinoid tumors, which cannot be managed endoscopically
Aggressive resection
Large and invasive sporadic type 3 carcinoid
Numerous small lesions that cannot be managed conservatively
Prognosis
Patients with lesions < 2 cm or those confined to mucosa or submucosa fare well, irrelevant of type
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


