Carcinoid Tumor, Appendix
Scott R. Owens, MD
Key Facts
Clinical Issues
Found in up to 1.5% of patients undergoing appendectomy
Appendiceal CTs occur at younger mean age than CTs in rest of gastrointestinal tract
When symptomatic, can present with acute appendicitis
Macroscopic Features
Most common (70-80%) in appendiceal tip
Routine longitudinal section of appendiceal tip essential in finding incidental tumors
Proximal margin status should be documented
Microscopic Pathology
Nests and cords of neoplastic neuroendocrine cells, often with peripheral palisading
Both tubular carcinoid and clear cell carcinoid are morphological variants that have similar clinical behavior to conventional CT
Top Differential Diagnoses
Goblet cell carcinoid
Distinction of conventional CT from goblet cell carcinoid essential as latter much more aggressive
Diagnostic Checklist
Subtle tumors may be difficult to see at low magnification
Tumors may be easy to overlook and should be actively sought in “routine” appendectomy specimens, particularly those with acute appendicitis
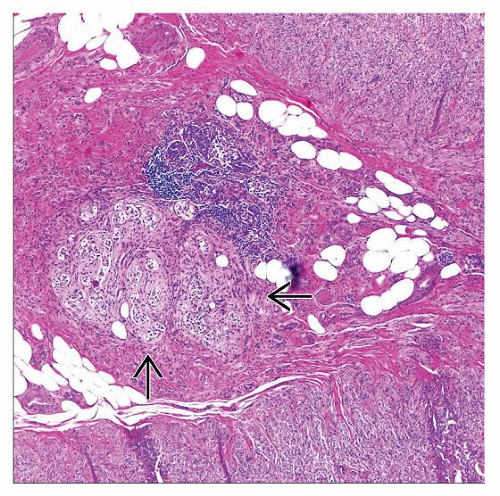 Hematoxylin & eosin shows carcinoid tumor  in an appendiceal tip with fibrous obliteration. Tumor nests are also present in the muscularis propria but are difficult to see at this magnification. in an appendiceal tip with fibrous obliteration. Tumor nests are also present in the muscularis propria but are difficult to see at this magnification. |
 Synaptophysin stain shows infiltrating nests of carcinoid tumor. Note the extensive infiltration of small nests in the left half of the field. |
TERMINOLOGY
Abbreviations
Carcinoid tumor (CT)
Synonyms
Well-differentiated neuroendocrine tumor (neoplasm)
Well-differentiated neuroendocrine carcinoma
Definitions
CT: Neoplastic proliferation of (usually) ECC with variable but frequently indolent clinical behavior
ECC: Gastrointestinal neuroendocrine cells that produce serotonin
CLINICAL ISSUES
Epidemiology
Incidence
Account for as many as 75-85% of all appendiceal tumors
Found in up to 1.5% of patients undergoing appendectomy
Age
Wide age range; common childhood gastrointestinal neoplasm
Appendiceal CTs occur at younger mean age than CTs in rest of gastrointestinal tract
Gender
M < F (especially in older age group)
Presentation
Most often incidental/asymptomatic
Abdominal pain
When symptomatic, can present with acute appendicitis
Caused by luminal obstruction by tumor
“Carcinoid syndrome”
Only occurs in “functional” (i.e., serotonin-producing) cases with metastasis, allowing vasoactive substances into systemic circulation
Diarrhea, flushing, asthma
Treatment
Surgical approaches
Appendectomy sufficient for small tumors confined to appendix
Margin status important
Larger tumors (> 2.5 cm) or those that spread beyond appendix may require right hemicolectomy
Includes those with positive margin(s) &/or spread into mesoappendix, regional lymph nodes
Survival benefit of this approach, especially when based solely on size, is controversial
Prognosis
5-year survival = 85%
Survival > 95% (as high as 99% reported) if tumor confined to appendix
Larger &/or more aggressive tumors (angiolymphatic spread, regional or distant metastasis) have lower survival
MACROSCOPIC FEATURES
General Features
Most common (70-80%) in appendiceal tip
Fewer (˜ 20%) occur in appendiceal body
Rarely occur in base of appendix
May reflect distribution of putative cell of origin (Kultschitzky cell)
Submucosal cell with endocrine and neural features
May appear as yellow or tan stellate nodule or area of mural thickening
Regional lymph node metastasis occurs in 4-5%
Sections to Be Submitted
Routine longitudinal section of appendiceal tip essential to find incidental tumors
Proximal margin status should be documented
MICROSCOPIC PATHOLOGY
Key Descriptors
Predominant pattern/injury type
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


