Chapter 9 Cancer
Cancer — what is it?
Various other terms, apart from cancer, are used to describe this family of diseases that include malignancy and neoplasia. The difference between a malignant and benign tumour is summarised in Table 9.1.
Table 9.1 Differences between benign and malignant tumours
| Benign | Malignant |
|---|---|
Cancer cells are invasive and are not restricted to normal boundaries, therefore they destroy adjacent tissues. These cells survive beyond the limitations of normal cells. The telomere shortening that occurs at the end of chromosomes in normal cells is not seen in cancerous cells.1
Cancer cells can either be differentiated (Grade 1) or undifferentiated (Grade 3). In general, the differentiated cells are associated with normal immunity, whereas the undifferentiated ones are associated with poor immunity and, hence, the latter spread (metastases) more rapidly throughout the body.2
Cancer cells not only utilise lots of energy (a marked increase in glycolytic capacity) but also have a negative influence on metabolism, especially increased protein metabolism.3 Cancer cachexia, which is a loss of weight, muscle atrophy and loss of appetite, is not only due to poor intake, but also changes in metabolism.
How common is cancer?
Cancer can affect people of all ages. Over the course of a lifetime about every 1:2 males and 1:3 females in Australia and most Westernised countries will develop an invasive cancer.4, 5 The commonest cancer in males in 2005 in Australia was prostate cancer, and in females, breast cancer.4
The commonest cancers in males (in a descending order of frequency) are:
The commonest cancers in females (in a descending order of frequency) are:
The total numbers of cancers is increasing, this growth is due mainly to the ageing population.4 In males the top 5 cancers accounted for over 67% of all diagnoses, whereas in females, the top 5 cancers accounted for 63% of all diagnoses. When sexes are combined, the commonest cancer is prostate cancer.4 The 5 top cancers accounted for over 61% of all diagnoses.
The commonest internal cancers, sexes combined (in a descending order of frequency) are:
Almost all cancers occur at higher rates in males than females. The male rate is 1.4 times the female rate.4
Risk factors
In general, it is reasonable to assume that there is not 1 particular factor that is completely responsible for the cause of cancer, although 1 factor is likely to be more important than the others. It is most probable that cancer cells are formed on a regular basis, but they are destroyed when important mechanisms, such as immunity, are functioning normally and there are not excessive stimulatory hormones and other chemical insults that can destabilise immune and metabolic control.
The risk factors for cancer are:
Genetics (family history and ageing)
Most cancers are sporadic and have no strong hereditary basis. A large number of cancers have now been found to have a genetic link, but this is not the key factor leading to the development of the cancer.6 Genetic cancer research is being very actively researched with the hope of detecting those individuals who are at risk, and then being able to provide additional protection through lifestyle changes. Hopefully in the future, it may be possible to genetically engineer these genes with the aim of preventing cancer.
A number of cancers are recognised as syndromes of cancer that have a defective tumour suppressor allele.7 The following are examples: mutations in genes, BRCA1 and BRCA2 which are associated with an elevated risk of breast and ovarian cancers, and hereditary non-polyposis colorectal cancer (HNPCC), also known as the Lynch syndrome. Several genes are involved and include cancers of the colorectum, uterine, gastric and ovarian sites without preponderance of colorectal polyps. A range of genetic mutations and switches are activated which can initiate cancer.
Behavioural and social factors
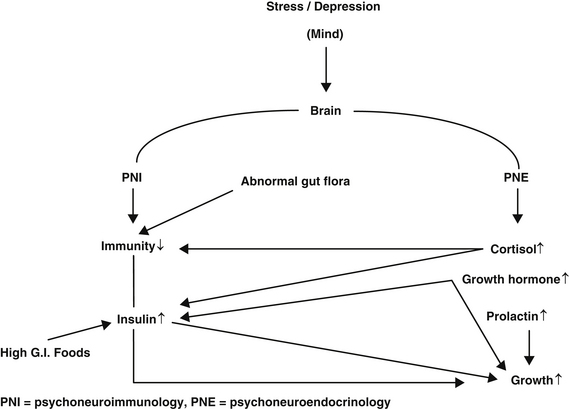
Psycho-oncology is the scientific field that describes the links between psychological and social factors with cancer. Depression is the key emotional factor that can influence immunity (psychoneuroimmunology (PNI)), as well as numerous hormones (psychoneuroendocrinology (PNE)). Depression can also influence lifestyle factors, including smoking, excess alcohol, physical activity and excess weight.8
The general overview of the key mechanisms involved in cancer are shown in Figure 9.1
An extensive review by David Spiegel concluded that chronic and severe depression is probably associated with an increased risk of developing cancer and the evidence was strong that depression predicts a poor prognosis, with more rapid progression of cancer.9 Risk of developing cancer due to depression is nearly doubled, independent of other lifestyle factors, and it is not related to any particular cancer.10, 11, 12
The longer the duration of depression the greater the risk for developing cancer.13 Depression and stress depress immunity and also increase levels of cortisol, growth hormone, prolactin and epinephrine, all of which are known to stimulate cancer growth.14–17
Insulin plus insulin-like growth factors (IGFs) have been shown in numerous epidemiological studies to be involved in increasing cancer risk.18, 19, 20 Stress can suppress natural killer cells leading to poor cancer surveillance in some cancers.21 There is increasing evidence that behaviour can influence our genes. Stress can damage DNA and impair genetic mutation repair.22, 23, 24
Personality factors, as well as sexual differences, are important relating to DNA damage.25 DNA damage is related to tension, anxiety and self-blame coping strategy in males, and in females, depression and rejection. The worst factor was the lack of subjective closeness to parents in childhood. DNA damage was also higher in subjects who had experienced the loss of a close family member within the last 3 years.
Immune cells have less ability to initiate genetically programmed cancer cell suicide with psychological stress.26 The repair of DNA is often depressed in cancer patients, which is a possible marker of cancer susceptibility.27
Shift work is associated with an increased risk of cancer which may be due to depleted melatonin levels.27 Melatonin is known to have a positive influence on immunity and also has anti-cancer effects.28, 29
Melatonin can inactivate cancer genes plus inhibits cancer growth factors.30
Inflammation and infection
Chronic inflammation is a central event that is closely associated with cancer development. Under normal circumstances, insulin has an anti-inflammatory action but this can be reversed with insulin resistance.31, 32
A recent study found that people with the highest blood levels of C-reactive protein were about 3 times more likely to develop colorectal cancer, as those with the lowest ranges.33 Elevated serum interleukin-6, which is another inflammatory marker, is also linked to cancer.34 The interesting chemo-prevention of cancer with COX-2 inhibitors is partially to do with this inflammatory process.35, 36, 37
Selective COX-2 inhibitors (Clecoxib and Rofecoxib) were used to prevent cancer with reasonable success, but withdrawn for this use because of serious side-effects.38, 39, 40
Curcumin, which is found in ginger and turmeric, is a COX-2 inhibitor and also has anti-cancer activity.41, 42 It is possible that the anti-inflammatory action of vitamin D is an important reason why it can protect from cancer.43, 44, 45 Inflammation associated with surgery can increase the size of metastases.46
Men with periodontal disease have been found to have 63% higher risk of pancreatic cancer compared to those with no sign of the disease.47 Inflammation is thought to be a key factor, but also higher levels of oral bacteria and higher levels of nitrosamines might also play a role. Other studies have shown that periodontal disease is a risk factor for other cancers.48, 49
Helicobacter pylori (H. pylori)
Stomach cancer is the second leading cause of cancer death worldwide, and approximately half of the world’s population is infected with H. pylori.50 Conventional triple therapy is now involved with a 20% failure. In addition to being expensive, it has significant side-effects.51, 52
On a global basis, there is geographic correlation between areas with high stomach mortality rates and high prevalence of H. pylori infection.53
Studies have reported an inverse association between vitamin C intake and gastric cancer risk.54 A randomised double-blind study from China was designed to reduce the prevalence of precancerous stomach lesions. This study had 3 groups, namely 3365 eligible participants that were randomly assigned in a factorial design to 3 interventions or placebos: amoxicillin and omeprazole for 2 weeks in 1995, (H. pylori treatment); vitamin C, vitamin E, and selenium for 7.3 years (vitamin supplement); and aged garlic extract and steam-distilled garlic oil for 7.3 years (garlic supplement). The study concluded that the drug treatment group showed a protective effect against pre-malignancy and malignancy. The supplement groups did not show a positive response. The authors of this study agree that the quality and doses of supplements may have been inadequate.55
There have been numerous studies using in vitro, animal and human groups dealing with H. pylori and probiotics, which have been summarised by Vitetta and Sali.56 In vitro probiotics inhibit H. pylori infection and all studies show that probiotics can reduce H. pylori gastritis and reduce the number of H. pylori.56
Seven of 9 human studies showed an improvement of H. pylori-induced gastritis and a decrease of H. pylori density following administration of probiotics.56 The addition of probiotics to standard antibiotic treatment improved H. pylori eradication and H. pylori therapy-associated side-effects.57
Olive oil polyphenols have in vitro activity against H. pylori and hence have the potential of being a chemo-preventive agent for peptic ulcer or gastric cancer.58
Viruses and cancer
Hepatitis virus B and C (HBV and HCV)
Several epidemiologic and experimental studies have established a causal role for HBV and HCV in the development of hepatocellular carcinoma.50, 59, 60
Patients with cirrhosis develop nutritional deficiencies and subsequent immunologic problems. These factors could be part of the reason why these patients are at an increased risk to develop liver cancer.61 Specific nutrient deficiencies have also been found in those with liver cirrhosis such as impaired vitamin E status, reduced carotenoids and lipid soluble vitamins.62, 63, 64
Vegetable, fruit and antioxidant nutrient consumption has been found to be associated with decreased subsequent risk of hepatocellular carcinoma.65 This group found that consumption of vegetables, green-yellow and green leafy vegetables were inversely associated with the risk of hepatocellular cancer.
Curcumin has been found to inhibit hepatic fibrosis in the rodent model, and may offer protection from subsequent hepatocellular carcinoma development.66
Sho-saiko-to, a traditional Japanese herbal formula, has been shown to play a chemo-preventive role in the prevention of hepatocellular carcinoma in cirrhotic patients.67
Human papilloma viruses (HPVs)
HPVs are DNA viruses that have been causally linked to cancers of the cervix and are suspected to be causally related to anal cancers and cancers of the aerodigestive tract.50, 68, 69
Apart from smoking, dietary factors appear to modulate cervical cancer.70 Women consuming low levels of vitamin C and carotenoids are at increased risk of cervical neoplasia, vitamin E and folate may also provide protection. Another study found that a diet high in folate, riboflavin, thiamine and vitamin B12 may play a protective role in cervical carcinogenesis.71 It is possible that these nutrients may help reverse cervical dysplasia.
Elevated serum homocysteine levels are strongly significantly predictive of invasive cervical cancer risk; folate, B6 and B12 are known to reduce homocysteine.72 Vegetable consumption and an increase in circulating cis-lycopene were protective against HPV persistence in another study.73
Dietary factors
It is now understood that the development of most cancers is clearly a result of an intimate interaction between endogenous and lifestyle factors, the most notable of these lifestyle factors is diet. Estimates suggest that approximately 30% of cancers are a consequence of suboptimal diet.74, 75, 76 In developing countries, the contribution of diet to cancer is estimated to be lower (20%) based mainly on higher tobacco consumption.77
Our food and drink contain mutagens and carcinogens in addition to a variety of chemicals that may be able to block carcinogenesis.78 Epidemiological investigations have been very helpful in defining the general profile of the diet which is protective: one which is low in red meat and various fats, modest in calories and alcohol, and high in fruit, vegetables and fibre. It is quite clear that a diet high in fresh fruits and vegetables is highly protective against colorectal cancer.79, 80
It is important to note that nutrition plays a role in influencing the body in many ways (e.g. immunity, behaviour) and, hence, it is likely that it plays some part in the development of all cancers, even where there is no data available. Most of the data relating to cancer and nutrition is for the more common cancers, and it is likely that a food that is good or bad for 1 cancer will be good or bad for another cancer.
Carcinogens in food
The importance of dietary acrylamide and its association with human cancers remains controversial.81, 82, 83
In 2002, Swedish scientists reported the presence of acrylamide in carbohydrate-rich foods that were produced at high temperatures, such as French fries, potato chips, breakfast cereals and toasted bread.84 Studies have shown positive dose-response relations to acrylamide exposure and cancer in multiple organs in both mice and rats.85, 86
Xenoestrogens
Xenoestrogens are defined as chemicals that mimic some structural parts of the physiological oestrogen compounds, therefore may act as oestrogens or could interfere with the actions of endogenous oestrogens. Organochlorine chemicals — pesticides, polychlorinated biphenyl compounds and other members of the Dioxin family are regarded as xenoestrogens or ‘endocrine disruptors’. These chemicals are capable of modulating hormonally unregulated processes including changes in growth factors that may be responsible for carcinogenesis, as well as congenital defects plus infertility in males.87, 88, 89
There is still controversy as to how significant the role of xenoestrogens are in humans.90
Chlorine
In population-based case-controlled studies, chlorine in water, which is the most important and the most common disinfectant, has been linked to several cancers including bladder, colorectal and possibly brain cancer.91, 92, 93 The risk is higher with more tap water that is consumed. Another group found that drinking chlorinated water disinfection by-products increased the risk of chronic myeloid leukaemia with increasing years of exposure.94
It was unusual that a protective effect was noted for chronic lymphoid leukaemia.93
Arsenic
Ingestion of inorganic arsenic from drinking water has emerged as an important factor in the cause of lung, bladder and non-melanoma skin cancers and possibly other cancers.95, 96 High levels of inorganic arsenic are found in the drinking water of many countries, including China, Argentina, Finland, Hungary and the US.95, 96
For a summary of dietary factors in cancer risk see Table 9.2.
Table 9.2 Dietary constituents reported to raise or lower the risk of cancer74, 97
| Dietary constituents in cancer | ||
|---|---|---|
Environmental factors
Air pollution
Long-term exposure to combustion-related air pollution is known to increase the risk of lung cancer, being higher in the more polluted cities.98 The cancer risks of organic hazardous air pollutants in the US have been ranked.99 Most of the polycyclic aromatic hydrocarbon, benzene, acetaldehyde and 1,3-butadiene risk was found to come from outdoor sources, whereas indoor sources were primarily responsible for chloroform, formaldehyde, and naphthalene risks.99
Electromagnetic fields (EMFs)
An advisory panel to the US and National Institutes of Science challenged a 1996 panel from the same institutes which said they found no conclusive evidence that EMFs generated by power lines and appliances were a threat to humans.100
The more recent panel found that children living near power lines appeared to have a 50% risk of leukaemia and adults had a similar increased risk of leukaemia if they were exposed to high levels of EMFs from utilities in their work places.100
A Tasmanian study has investigated residential exposure to electric transmission lines and risk of cancer.101 This case-controlled study found that there is a possibility that residents close to high voltage power lines, especially early in life, may increase the risk of myeloproliferative and lymphoproliferative disorders. Further larger, independent studies are required to be more conclusive about this issue.
In developed countries, people are constantly being irradiated from numerous sources including phones, internet, wireless, various kitchen appliances (e.g. microwave ovens and electric blankets), and it remains controversial as to whether this exposure produces adverse health effects. It is possible that EMFs may interfere with melatonin secretion.102, 103
A case-controlled study of 1700 workers employed as electricians and exposed to electric fields showed no increase in leukaemia, but there was an increase in brain tumours (no specific type), as well as colorectal cancer.104
Genetically modified foods (GM foods)
Current research in GM foods is contradictory and inconclusive, and includes much evidence showing potential health risks.105 Compass cases of adverse reactions to GM crops in humans have been recorded ranging from allergies following skin contact to an outbreak of unprecedented disease affecting thousands and dubbed eoseniamyalgia.106, 107
It is controversial whether GM crops can produce higher yields. There is also evidence showing that non-GM crops using natural matters can increase crop yield.108 There is insufficient data to do with the long-term effects of GM foods on human health.
Ionising radiation
Most people are unaware that the greatest source of exposure to ionising radiation is background radiation in the environment, which constitutes 82% of all exposure (see Figure 9.2).109
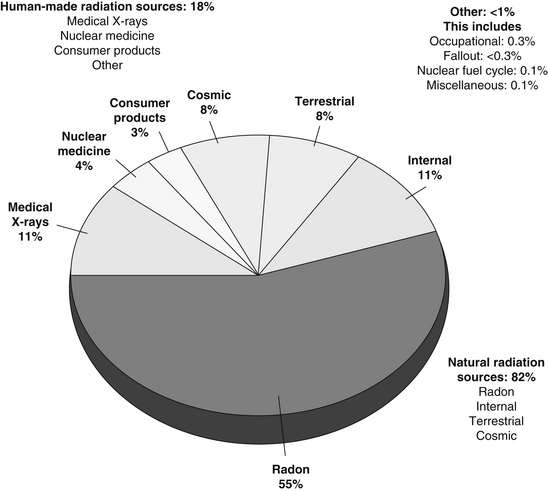
Figure 9.2 Ionising radiation exposure to the public
(Source: Nasca PC, Pastides H 2008 Fundamentals of Cancer Epidemiology. Jones and Bartlett Publishers, Boston)
Medical radiation is the largest source of human-made radiation and exposure is continuing to increase with time.110 X-ray treatment for ankylosing spondylitis increases the risk of leukaemia, radiation for menorrhagia leads to a threefold risk of leukaemia, and radiotherapy to cancer patients has been clearly shown to increase the risk of developing secondary cancers.111, 112, 113 The thyroid is particularly sensitive to ionising radiation, especially when given to children.114
A recent retrospective study found that thyroid cancer patients with exposure to radiation from health care work places, or treatments for conditions such as breast cancer and acne, appeared to have worse outcomes than patients with the disease and no exposure.115 The use of computer tomography (CT) scans is of real concern, as studies demonstrate that radiation exposure from CT coronary angiography is a risk for cancer.116 Melbourne radiologists have called for a curb on CT scans unless completely essential.117
Toxic chemicals
Pesticides, weed–killers
It is estimated that there are about 80 000 toxic chemicals in use at present, with about 5000 used extensively.118, 119, 120
An environmental history from a patient investigates the following areas of exposure:
Some examples of toxic chemicals include dioxins and bisphenol-A (BPA).
Dioxins
A number of disorders are associated with exposure to dioxins including learning disabilities, infertility, endometriosis, immune dysfunction, endocrine disruption and carcinogen. High levels are found in large fish such as sharks, marlin and swordfish, as well as in breastmilk.120
Bisphenol–A (BPA)
Recent investigations have shown that BPA has oestrogenic activity which can lead to miscarriage, birth defects, disruption of beta cells of the pancreas, thyroid hormone disruption, liver damage plus obesity-promoting effects.121 This study also found an association of elevated urinary BPA with cardiovascular disease, diabetes and abnormal liver function tests. BPA is commonly used to line baby’s milk bottles, as well as food cans.121
Occupational exposure
Diesel exhaust fumes in trucking industry workers
Trucking industry workers who have regular exposure to diesel vehicle exhaust and other types of vehicles on highways, city streets, and loading docks have an elevated risk of lung cancer with increasing years of work.122
Exposure to pesticides
Brain tumours have been associated with several occupational and environmental exposures.123, 124, 125
Some pesticides contain alkylureas or amines that metabolise to nitroso compounds which have been associated with neurogenic tumours.126 However, a more recent study investigating exposure to pesticides and risk of adult brain tumours did not find an association between herbicide or insecticide exposure among men.123 Women with occupational exposure to herbicides had an increased risk of meningioma.123
Exposure to the styrene-butadiene rubber industry
An epidemiological study of 17 000 workers in the rubber industry found an increased risk of chronic lymphocytic and myelogenous leukaemia in the most highly exposed workers.127 Furthermore, in a study of workers involved in butadiene-monomer production, an association with non-Hodgkin’s lymphoma was found.128
Ethylene oxide
This chemical is used in the production of other chemicals although most human exposure occurs from its use in sterilisation of medical equipment. An increase in breast cancer occurs with a significant exposure-response relationship between ethylene oxide exposure and breast cancer incidence.129
Vinyl chloride exposure
Two large multi-centre cohort studies in facilities that manufactured vinyl chloride, polyvinyl chloride or polyvinyl chloride products showed a substantial increase in the relative risk for liver and gliosarcoma with risk increasing with duration of exposure or total exposure.130, 131
Hair dyes
Personal use of hair dyes may play a role in the risk of follicular lymphoma and chronic lymphatic leukaemia plus small lymphocytic leukaemia.132 A meta-analysis of epidemiological data has found that personal use of hair dyes is associated with an increased risk of bladder cancer.133
Cooking oil fumes
Fumes from 6 different oils: safflower, olive, coconut, mustard, vegetable and corn have been collected and polycyclic aromatic hydrocarbons (PAHS) were extracted from air samples.134 Fumes from safflower oil, vegetable oil and corn oil were found to have PAHS. It is thought that PAHS fumes are linked to lung cancer.
Risks to fire fighters
A review of 32 studies on fire fighters, which was to determine cancer risk using a meta-analysis, has found that there is an elevated risk of multiple myeloma.135 In addition, a probable association with non-Hodgkin’s lymphoma, prostate and testicular cancer was demonstrated.
Sleep patterns
Both short and long sleep duration have been associated with increased mortality from all causes for both sexes, yielding a u-shaped relationship with total mortality and a nadir at 7 hours of sleep.136 It is also of significance that usage of hypnotics is associated with an increased all-cause mortality and cause a specific mortality in regular users of hypnotics.137
It is not surprising that lack of sleep disturbance can influence mortality, as it is closely associated with stress and depression which, in turn, are linked to cancer and cardiovascular disease. Short sleep duration is also associated independently with weight gain and the latter is a risk factor for a number of cancers.138, 139, 140
Studies have found that increased sleep duration is associated with a decreased risk of breast cancer.141, 142
The frequent occurrence of disturbed sleep in cancer patients is of great concern, as many of these patients may already be suffering from fatigue due to psychological factors, chemotherapy, cancer pain or general debilitation.143 It is essential to enquire about sleep in cancer patients and to ensure that sleep disturbance is managed properly. The patient’s quality of life and their tolerance to treatment, as well as the development of mood disorders is dependent on adequate sleep.143
It is controversial whether the level of melatonin is strongly associated with the risk of breast cancer.141, 144
Exercise and cancer
Cancer prevention
The protective effect of regular exercise has been demonstrated in a number of cancers including breast, colorectal, prostate, testicular and lung cancer.145, 146, 147 There is also evidence that exercise may offer protection against endometrial, ovarian and also other forms of cancer.145, 148, 149
Exercise is known to improve immunity in the following ways:
A large study of 30 000 men found that unless they were extremely obese, cardiorespiratory fitness can abolish the risk of dying of cancer associated with being overweight.157
In the US, the surgeon general recommends 30 minutes a day of exercise most days of the week, which is generally accepted as 5 days of the week for a total of 150 minutes a week.158, 159
Resistance exercise may also be protective, as it can reduce insulin resistance in a similar way to aerobic exercise.160, 161
Cancer survival
Regular exercise can improve survival in colorectal and breast cancer patients, 50–60%.162, 163
A study of 3000 women with various stages of breast cancer were followed for 18 years and those who walked 3–5 hours per week had twice the survival than those who did not exercise.163 A further study in women with breast cancer, followed up for a period of 9 years, who exercised regularly had a 44% reduction in mortality.164 A group of 500 colorectal cancer patients were found to have half the mortality if they exercised regularly.162
In a very large prospective study of nearly 48 000 men, of the men over 65 years of age 3000 developed prostate cancer. Those who exercised regularly had reduced their chance of developing an aggressive cancer by two-thirds compared to the men who did not exercise.165
A meta-analysis of cancer survival following chemotherapy in cancer patients by Morgan and others, found that survival was improved by 2% in 5 years, which is minimal compared to the benefits of exercise.166
Exercise used during cancer treatment can counteract side-effects of disease and treatments.167 Twice weekly resistant training appears to be safe and well-tolerated, resulting in increased muscle mass and decreased body fat.168 Resistance exercise, particularly useful in men receiving androgen deprivation therapy for prostate cancer, resulted in improved quality of life and muscular fitness.160
Cancer fatigue
Exercise may also reduce fatigue resulting from chemotherapy, in cancer patients. Regular exercise can increase the fitness in breast cancer patients treated with conventional chemotherapy.169
The relative importance of cancer fatigue has been compared with other patient symptoms and concerns over 9 cancer types, and emerged as the top-rated symptom.170 To explore this issue, the author surveyed 534 patients and 91 physician experts from 5 institutions and community support agencies. It was thought by most that fatigue was attributable to both disease and treatments. Sleep disorders and difficulty falling asleep, problems maintaining sleep, poor sleep efficacy, early awakening and excessive daytime sleep are prevalent in cancer patients.171 Cancer fatigue can be modified by ensuring optimum sleep quality.172 Exercise and counselling may help to reduce fatigue.173
Overweight and obesity
The increasing incidence of obesity throughout most Western countries is said to impose a major additional cancer burden at a time when population ageing is projected to cause unprecedented growth in cancer incidence.174, 175
While obesity is frequently associated with type 2 diabetes, hypertension, lipids abnormalities and death from heart disease and stroke, there is growing evidence of its role in causing cancer. A systematic review and meta-analysis, which included the Million Women Study, investigated the link between body mass index (BMI; calculated by dividing weight in kilograms by height in metres squared) and types of cancer.176, 177
In men, a 5 kg per metre squared increase in BMI was strongly associated with adenocarcinoma of the oesophagus, thyroid, colon and renal cancers, and in women with adenocarcinoma of the oesophagus, endometrial, gall bladder and renal cancers. There were weaker associations for melanoma and rectal cancer in men, and post-menopausal breast, thyroid and colon cancer in women. Leukaemia, myeloma and Hodgkin’s disease were associated in both sexes. Another study found higher risks of oesophageal and gastric cardia adenocarcinoma with increasing BMI.178
It is uncertain if obesity is related to prostate cancer.179 Recent evidence suggests that obesity increases risk of advanced prostate cancer and prostate cancer mortality, but not the risk of less aggressive disease.179
Many nutritional factors are also associated with aggressive and fatal prostate cancer.196 Furthermore, greater plasma insulin-like growth factor, 1 level (IGF-1), is associated with a fivefold increased risk of advanced stage prostate cancer, but was not associated with early-stage prostate cancer.180 It is of interest that insulin receptors are present on primary human prostate cancers.181
A possible mechanism for the association of obesity and cancer is that chronic insulinaemia results in raised levels of 3 IGF-1, with higher mean concentration in men compared to women. The raised level of free IGF-1 alters the environment of cells to favour cancers developing.182
Autocrine stimulation of the growth factor receptor (IGF-IR) by IGF-22 is 1 mechanism that allows cancer cells to maintain unregulated growth and to resist program cell death (PCD).183 Obesity and type 2 diabetes are generally independently associated with an increased risk of developing cancer and a worse prognosis.184 The etiology is yet to be determined, but insulin resistance and hyperinsulinaemia may be important factors. Hyperglycaemia, hyperlipidaemia and inflammatory cytokines in addition to IGFs are also possible factors involved in the process.
A study has found that patients with elevated insulin or glucose at the time of colorectal adenoma removal are at increased risk of recurrent adenoma.185 Those with an increased glucose and an increased risk for recurrence of advanced adenomas, however a systematic review meta-analysis investigating the association of glycaemic index (GI) and glycaemic load (GL) intakes with the risk of digestive tract neoplasms found that neither GI or GL intakes were associated with colorectal or pancreatic cancers.186 In contrast, results from the very large Nurses Health Study showed that high GL and insulin resistance combined to increase pancreatic cancer risk.187
It is known that diabetes diagnosed 5 or more years prior to cancer detection was associated with a twofold increasing risk of pancreatic cancer; another study found a 50% increase for diabetes diagnosed 10 or more years prior to cancer detection.188, 189 Numerous studies show that overweight individuals are consistently at high risk of pancreatic cancer compared to leaner individuals.190, 191
The association between body weight and diabetes suggests that insulin resistance may play a role in pancreatic carcinogenesis. A systematic review and meta-analysis of dietary GI, GL and breast cancer by the same group did not provide strong support of an association between dietary GI and GL and breast cancer risk.192 Another meta-analysis found that low GI and/or low GL diets were independently associated with reduced risk for heart disease and diabetes.193
A Cochrane review demonstrated a low GI and GL diet reduced body mass and improved lipids profiles.194
In comparison, a large Swedish study of more than 60 000 women over a 20-year period found that when women were overweight they had signs of insulin resistance — such as elevated blood glucose or insulin levels, they were about 50% more likely to be diagnosed with an advanced breast cancer.195
In contrast, another meta-analysis of dietary GI, GL and endometrial plus ovarian cancer showed that a high GI, but not a high GL diet, is positively associated with a risk of endometrial cancer, particularly among obese women.190
A retrospective study found that diabetes is a significant predictor of tumour recurrence after potentially curative therapy for hepatocellular carcinoma.196
Obesity appears to not be associated with prostate cancer, but studies have suggested that obese men are more likely to develop aggressive and fatal prostate cancer.197, 198 Beneficial effects of exercise in reducing colorectal, breast and prostate cancer may be through reducing hyperinsulinaemia and via IGF access.199, 200
Methological issues might explain the failure to detect differences between high and low GI diets.201 There are always difficulties in collecting accurate dietary information which would allow for the accurate calculation of GI and GL, which in turn influences the results of these studies.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


