Chapter 8 Breast disease and breast cancer
Benign breast diseases
The phrase benign breast diseases encompasses a heterogeneous group of lesions that may present a wide range of symptoms or may be detected as attendant microscopic findings. The incidence of benign breast lesions begins to rise during the second decade of life and peaks in the 4th and 5th decades, as opposed to malignant diseases, for which the incidence continues to increase after menopause, although at a significant less rapid pace1, 2, 3
The majority of the lesions that occur in the breast are benign4 and are far more frequent than malignant ones5, 6, 7 With the advent of screening techniques such as mammography, ultrasound, and magnetic resonance imaging of the breast and the extensive use of needle biopsies, the diagnosis of a benign breast disease can be accomplished without surgery in the majority of patients.
The most frequently seen benign lesions of the breast have been summarised as developmental abnormalities, inflammatory lesions, fibrocystic changes, stromal lesions, and neoplasms (see Table 8.1).
Table 8.1 Benign and malignant conditions of the breast4
| Benign breast conditions |
|---|
Inflammatory and related lesions |
| Malignant breast conditions |
Benign breast conditions — fibrocystic breast changes
Fibrocystic breast conditions (FBC) are the most common benign breast problem encountered in women. The following characteristics have been reported:8
Treatment (or management) of FBC
Lifestyle
Lifestyle changes that may be helpful include exercise, which may decrease breast tenderness. In 1study, women who walked approximately 30 minutes on most days reported less breast tenderness as well as improvement in other symptoms, such as anxiety.8
Diets
Some studies have reported that women with FBC drink more coffee than women without the disease,9, 10 whereas other studies do not.11, 12 Eliminating caffeine for less than 6 months does not appear to be effective at reducing symptoms of FBC.13, 14 However, long-term and complete avoidance of caffeine does reduce symptoms of FBC.15, 16 Some women are more sensitive to effects of caffeine than others, so benefits of restricting caffeine are likely to vary from woman to woman. Caffeine is found in coffee, black tea, green tea, cola drinks, chocolate, and many over-the-counter drugs. A decrease in breast tenderness can take 6 months or more to occur after caffeine is eliminated. Breast lumpiness may not go away, but the pain often decreases.
FBC has been linked to excess oestrogen. When women with FBC were put on a low-fat diet, their oestrogen levels decreased.17, 18 After 3–6 months, the pain and lumpiness also decreased.19,20 The link between dietary fat and symptoms appears to be most strongly related to saturated fat.21 Foods high in saturated fat include meat and dairy products. Fish, non-fat dairy, and tofu are replacements to consider.
A recent study from the Women’s Health Initiative Dietary Modification trial investigated a total of 48 835 post-menopausal women, aged 50–79 years, without prior breast cancer.22 Participants were randomly assigned to the dietary modification intervention group or to the comparison group. The intervention was designed to reduce total dietary fat intake to 20% of total energy intake, and to increase fruit and vegetable intake to ≥5 servings per day and intake of grain products to ≥6 servings per day. Risk for developing benign breast disease varied by levels of baseline total vitamin D intake but it varied little by levels of other baseline variables. Hence, the results suggested that a modest reduction in fat intake and increase in fruit, vegetable, and grain intake do not alter the risk of benign proliferative breast disease. It is difficult to conclude about the importance of diet in such a study without knowing details relating to other lifestyle factors, such as behavioural and exercise habits.
Supplements
Omega-6 fatty acids
In a double-blind research trial, evening primrose oil (EPO) reduced symptoms of FBC,23 though only moderately. One group of researchers reported that EPO normalises blood levels of fatty acids in women with FBC.24 However, even these scientists had difficulty linking the improvement in lab tests with an actual reduction in symptoms. Nonetheless, most reports continue to show at least some reduction in symptoms resulting from EPO supplementation with doses of 3g/day of EPO for at least 6 months to alleviate symptoms of FBC.25, 26
Vitamins
While several studies report that 200–600IU of vitamin E per day, taken for several months, reduces symptoms of FBD,27, 28 most double-blind trials have found that vitamin E does not relieve FBC symptoms.29, 30
Vitamin B6
As with vitamin E, the effectiveness of vitamin B6 remains uncertain. The reduction of symptoms by vitamin B6 supplementation is controversial.31, 32 Since vitamin B6 supplementation is effective for relieving the symptoms of premenstrual syndrome (PMS), in addition to breast tenderness, women should discuss the use of vitamin B6 with their health care provider.
Herbal medicines
Vitex agnus castus (Chasteberry)
In 1 double-blind trial, a liquid preparation containing 32.4mg of Vitex agnus castus (VAC) and homeopathic ingredients was found to successfully reduce breast tenderness associated with the menstrual cycle (e.g. cyclic mastalgia).34 VAC is thought to reduce breast tenderness at menses because of its ability to reduce elevated levels of the hormone prolactin.35
Breast cancer — risk modification for prevention
Weight control and energy intake
There are numerous studies that report that controlling weight gain by reducing energy intake is associated with prevention of breast cancer.36, 37 Weight gain in adult life is an important risk factor for breast cancer. Observational studies indicate that pre-menopausal or post-menopausal weight loss is associated with a reduction in risk of post-menopausal breast cancer.38 On current scientific evidence the overall perception is that epidemiologic studies provide sufficient evidence that obesity is a risk factor for both cancer incidence and mortality.39 Moreover, the evidence supports strong links of obesity with the risk for cancer of the breast (in post-menopausal women) as well as numerous other malignancies.40
Environmental factors
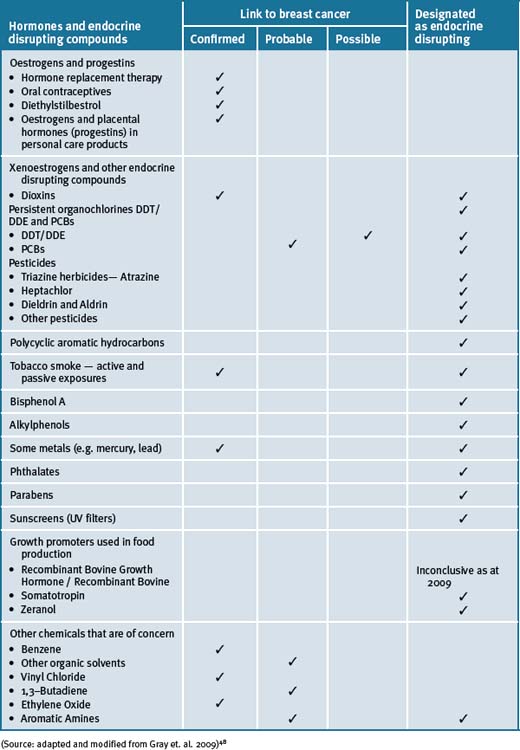
An increasing body of scientific evidence from both human and animal models indicates that exposure of fetuses, young children and adolescents to radiation and or environmental chemicals puts them at considerably higher risk for developing breast cancer in later life.41 These data are consistent with the role of environmental exposures, especially at young ages, in affecting the later incidence of breast cancer in women who have immigrated to relatively industrialised areas from regions of the world with lower risks of breast cancer. There are numerous environmental chemicals that have been associated with breast cancer (see Table 8.2).
The increasing incidence of breast cancer in the decades following World War II paralleled the proliferation of synthetic chemicals. An estimated 80 000 synthetic chemicals have been documented to be in use today in the US, and another 1000 or more are added each year.42 A recent survey indicated that 216 chemicals and radiation sources have been registered by international and national regulatory agencies as being experimentally implicated in breast cancer causation.43, 44 Many of the chemicals (i.e. that include common fuels, solvents and industrial processes) can persist in the environment45 and can accumulate in body fat and may remain in breast tissue for decades.46, 47
Nutritional influences
Soy and phytoestrogens
Phytoestrogens present in soy are structurally and functionally similar to oestrogen and have hence received significant attention as potential dietary modifiers of breast cancer risk. A meta-analysis of published studies on soy intake and breast cancer noted a significant protective effect of high soy intake on risk of breast cancer.49 The comparatively high dietary intake of soy in Asian countries has been hypothesised to at least partly explain the lower breast cancer incidence patterns in these countries as compared with the Western world. The hypothesis is however contentious.50, 51
A variety of health benefits, including protection against breast cancer, have been attributed to soy food consumption, primarily because of the soybean isoflavones (genistein, daidzein, glycitein).52 Isoflavones are considered to be possible selective oestrogen receptor modulators but possess non-hormonal properties that also may contribute to their effects.
A recent RCT study did not support the hypothesis however, that soy intake reduced breast cancer risk.53 A diet high in soy protein among post-menopausal women did not decrease mammographic density. A further recent study from Japan supports this notion.54 This prospective study suggested that consumption of soy food had no protective effects against breast cancer and that large-scale investigations eliciting genetic factors may clarify different roles of various soybean-ingredient foods on the risk of breast cancer.
Moreover, no effect on menopausal symptoms was reported in a RCT that investigated oral soy supplements versus placebo for the treatment of menopausal symptoms in patients with early breast cancer.55
It has been proposed though that intake of soy in early life and or in adolescence may be protective for the later development of breast cancer.56 In most Asian countries where the incidence of breast cancer is exceptionally low, soy is consumed 2–3 times daily, and hence it is likely that it is protective.57
Dairy foods
There have been 3 meta-analysis published that have investigated the relationship between dairy food consumption and the risk of breast cancers. The first meta-analysis to combine the results of 5 cohort and 12 case-control studies about dairy product consumption and breast cancer risk found a small increased risk of breast cancer in women with greater intakes of milk.58
In 2002, and forming part of the Pooling Project, a pooled analysis of 8 cohort studies was published.59 For this pooled analysis, 8 prospective studies with at least 200 cases of breast cancers each were included, thus bringing a total of 351041 healthy women and 7379 invasive breast cancer cases to the analysis. With respect to dairy products, different food groups were considered. Dairy products were divided into solids (butter and cheese) or liquids (milk, yoghurt, ice cream, etc.). Subgroups were also considered (whole, semi-skimmed or skimmed milk). Thus, ten different subgroups of dairy products were considered. Dairy product intake was analysed as a continuous variable (incrementally of 100g daily consumption for all products except butter and cream, and 10g for cream) and as categorical variable comparing higher versus lower quartiles of consumption. Other dietary and non-dietary factors associated with breast cancer were also considered, such as total energy, alcohol intake, parity, menopausal status and body mass index (BMI; i.e. level of obesity). Women in the 4th quartile of liquid dairy products consumed almost 630g of this kind of dairy product daily, whereas women in the first quartile consumed only 360g daily. No relationship was found between dairy product intake and breast cancer risk, neither treating dairy products as a continuous variable nor treating it as a categorical one. The research did not find statistically significant associations in any of the 10 subgroups of dairy products considered. The analysis concluded that, taking into account data of more than 350 000 women, there was no evidence that a diet rich in dairy products during middle or advanced age could increase or modify the risk of breast cancer in North American or European women.59
A more recent review about consumption of dairy products and risk of breast cancer concluded that published epidemiological data do not provide consistent evidence for an association between the consumption of dairy products and breast cancer risk.60 This study pointed out limitations that must be considered. Namely the moderate reliability of the methods used to assess dairy product intake, which could lead to some misclassifications. Also that consumption of dairy products may be associated with other dietary habits or other variable nutrient content of dairy products (such as vitamin D consumption through food fortifications) that could also influence breast cancer risk.59
Meat consumption
A hypothesis has been advanced that links red meat consumption to the induction of carcinogenesis through it’s highly bio-available iron content, growth-promoting hormones used in animal production, carcinogenic heterocyclic amines formed in cooking, and its specific fatty acid content.61, 62
A meta-analysis of case-control and cohort studies reported that there was a modest association of red meat intake with breast cancer incidence,63 but no association was noted in a pooled analysis of prospective studies.64 More recent reports from 2 large prospective cohorts noted an elevated risk with higher red meat consumption. In an analysis of the NHS II (n = 1021 cases that were predominantly pre-menopausal), a positive association between red meat and breast cancer risk was observed, especially for oestrogen receptor-negative and progesterone receptor-positive cancers,65 comparing more than 1.5 servings per day to 3 or fewer servings per week. In the UK Women’s Cohort Study (n = 678 cases), an increased risk of breast cancer was observed among women with a high red meat intake, with a 12% increase in risk per 50g increment of meat each day.66 A study of post-menopausal Danish women (n = 378 cases) showed an elevated risk of breast cancer in those women consuming red meat and processed meat (≥25g per day). This association was confined to women genetically susceptible to carcinogenic aromatic amines due to polymorphisms in N-acetyl transferase.67
Carbohydrates
A number of prospective cohort studies have not shown any consistent associations between total carbohydrate, glycaemic index, glycaemic load, and breast cancer risk, and most results have not been significant.68 However, these findings are not consistent with the association of refined carbohydrates and obesity in Western societies and the link to breast cancer which is opposite to findings in Asian countries (see under ‘Weight control and energy intake’ in this chapter).
Alcohol
Moderate alcohol consumption has been reported to increase sex steroid hormone levels and may interfere with folate metabolism, both of which are potential mechanisms for the observed associations of moderate alcohol intake with several forms of cancer, particularly breast and colorectal.69, 70
A meta-analysis of pooled cohort studies showed that there was a 10% increase in breast cancer risk for every 10g of alcohol consumed per day.71 A similar magnitude of association was noted in 2 pooled analyses.72 A dose-response relationship without a threshold effect has been reported, such that with even 1 drink per day was predictive of a modestly elevated risk for breast cancer.73, 74 Menopausal status and type of alcoholic drink do not seem to modify this association. However, an interaction between folate and alcohol intake suggests that an adequate folate intake (most commonly achieved by taking a multiple vitamin or folate supplement) appears to reduce or eliminate the excess risk due to alcohol consumption.75, 76
A recent descriptive study has reported that alcohol and breast cancer risk may be defined by oestrogen and progesterone receptor status.77 Moreover, the study supported the notion that alcohol was more strongly related to oestrogen positive than to oestrogen negative breast tumours. Furthermore, a further study concluded that although smoking was not related to asynchronous contralateral breast cancer, this study, the largest study of asynchronous contralateral breast cancer to date, demonstrated that alcohol was a risk factor for the disease, as it was for a first primary breast cancer.78
Diets
Mediterranean diet
An early review has pointed out that a number of cancers, such as cancer of the large bowel, breast and other hormonal dependent organs, are less frequent in Mediterranean countries than in northern Europe.79 It has been put forward that a low dietary intake of saturated fat, accompanied by a higher intake of unrefined carbohydrates, and possibly other protective nutrients (phytochemicals in fruits and vegetables) could be the cause of such risk differences.
Recent studies suggested that adherence to a Mediterranean diet may be protective against breast cancer. An Italian study reported that a traditional Mediterranean diet significantly reduced endogenous oestrogen.80 The results of this important study could eventually lead to identifying selected dietary components that more effectively can decrease oestrogen levels and, hence, provide a basis to develop dietary preventive measures for breast cancer. A US study confirms such notions by reporting that in their study, selected dietary patterns (such as those found in the Mediterranean diet) may be protective primarily in the presence of pro-carcinogenic compounds such as those found in tobacco smoke.81
Moreover, Western lifestyles, characterised by reduced physical activity and a diet rich in fat, refined carbohydrates, and animal protein is associated with high prevalence of overweight, metabolic syndrome, insulin resistance, and high plasma levels of several growth factors and sex hormones. Most of these factors are associated with breast cancer risk and, in breast cancer patients, with increased risk of recurrences. Such metabolic and endocrine imbalances can be favourably modified through comprehensive dietary modification, shifting from a Western to Mediterranean and macrobiotic diets.82
Vegetarian diets
A recent study strongly suggests that a diet characterised by a low intake of meat and/or starches and a high intake of legumes is associated with a reduced risk of breast cancer in Asian Americans.83
Further, a recent study investigated the associations of different dietary patterns (Western, Prudent, Native Mexican, Mediterranean, and Dieter) with the risk for breast cancer in Hispanic women (757 cases and 867 controls) and non-Hispanic white women (1524 cases and 1598 controls) from the Four-Corners Breast Cancer Study.84 The results showed that the Western (odds ratio for highest versus lowest quartile) and Prudent dietary patterns were associated with greater risk for breast cancer, and the Native Mexican and Mediterranean dietary patterns were associated with lower risk of breast cancer. Body mass index modified the associations of the Western diet and breast cancer among post-menopausal women and those of the Native Mexican diet among pre-menopausal women. Associations of dietary patterns with breast cancer risk varied by menopausal and body mass index status, but there was little difference in associations between non-Hispanic white and Hispanic women.
It has also been reported that nutrition for primary prevention of breast cancer by dietary means therefore relies on an individually tailored mixed diet, rich in basic foods and traditional manufacturing and cooking methods.85
Nutritional supplements
Multivitamins and/or minerals
The relationship between breast cancer and micronutrients is complex. It includes folate, vitamins, and carotenoids, and has been investigated in large prospective studies using biomarkers of intake. Two recent meta-analyses noted a possible protective effect by folate, especially among women who drank alcohol.86, 87
A recent systematic review of vitamin and mineral supplement use among US adults after cancer diagnosis reported that breast cancer survivors had the highest use.88
A recent double-blinded, randomly controlled, cross-over trial of multivitamins versus placebo in patients with breast cancer undergoing radiation therapy was undertaken to evaluate fatigue and quality of life.89 The study results showed that no significant changes were elicited with the use of multivitamins. Hence, multivitamins supplementation did not improve radiation-related fatigue in patients with breast cancer. Moreover, a recent report on multivitamin use and risk of cancer in the Women’s Health Initiative (WHI) cohorts showed that following a median follow-up of 8.0 and 7.9 years in the clinical trial and observational study cohorts, respectively, the WHI study provided convincing evidence that multivitamin use had no influence on the risk of common cancers, cardiovascular disease (CVD), or total mortality in post-menopausal women.90 However, this study did not include lifestyle factors such as behaviour and exercise and, hence, it is difficult to see how its findings could be conclusive. Moreover, the recent Framingham study found that elevated homocystine was the most important risk factor for CVD which is usually normalised by a multivitamin supplement.91
Vitamin D
Vitamin D, a fat-soluble pro-hormone, is synthesised in response to sunlight. It has been documented that experimental evidence suggests that vitamin D may reduce the risk of cancer through regulation of cellular proliferation and differentiation as well as inhibition of angiogenesis.92
There have been 10 descriptive studies that have investigated the relationship between vitamin D intake and breast cancer risk. Namely, 5 cohort studies 93–97 and 5 case control studies.98–102 Overall, the case control study of Knight et. al.99 examined sunlight exposure and intake of vitamin D-rich foods as well as vitamin D supplements at various ages (10–19, 20–29, 45–54 years). Sun exposure and use of vitamin D supplements or multivitamins between the ages of 10–19 and 20–29 were associated with reduced risk of breast cancer. Of the hospital-based case-control studies, Nunez et. al.96 and the cohort studies of John et. al.,90 Shin et. al.,91 and McCullough et. al.94 provided some evidence for inverse associations, while the results of most of the remaining studies were essentially null.
Vitamins E
A double-blind, placebo-controlled, cross-over randomised clinical trial reported a marginal statistical effect of vitamin E (dose used 800IU/day) in the treatment of hot flashes. The treatment duration was for 4 weeks of daily vitamin E consumption and was compared with placebo in 120 breast cancer patients.103 Vitamin E was associated with 1 less hot flash per person per day and did not induce any significant toxicity. A cross-over analysis showed that vitamin E was associated with a minimal decrease in hot flashes. There was no preference for use of vitamin E over placebo when participants were assessed at the end of the study. The study hence suggested that vitamin E at a dose of 800IU daily can be used because it is inexpensive and non-toxic and it might result in a slightly better relief of hot flashes than placebo. The scientific evidence is therefore limited. Thus, more clinical data are warranted and caution is advocated as vitamin E is not registered for this use. However, these studies did not elucidate whether the synthetic or the natural form of vitamin E was used and hence the conclusions reached may be controversial.
Vitamin A and/or vitamin a-analogs
Studies on specific carotenoid intake and breast cancer risk modulation are limited.104 The roles that carotenoids, retinol, and tocopherols may have in breast cancer aetiology remain complex and largely inconclusive.105 It has been suggested though that consumption of fruits and vegetables high in specific carotenoids and vitamins may be the best option that could reduce pre-menopausal breast cancer risk.101, 106 Recently the relationship between plasma carotenoids at enrolment and 1, 2 or 3, 4 and 6 years and breast cancer-free survival in the Women’s Healthy Eating and Living (WHEL) Study participants (N = 3043), who had been diagnosed with early-stage breast cancer, concluded that higher biological exposure to carotenoids, when assessed over the timeframe of the study, was associated with greater likelihood of breast cancer-free survival regardless of study group assignment.107
An early study administered vitamin A to randomly allocated patients (n = 100) with metastatic breast carcinoma treated by chemotherapy.108 The daily doses employed indefinitely ranged from 350 000 to 500 000IU according to body weight. There was noted a significant increase in the complete response rate. When subgroups determined by menopausal status were considered in the analysis of the data, it was observed that serum retinol levels were only significantly increased in the post-menopausal group on high dose Vitamin A. Response rates, duration of response and projected survival were only significantly increased in this subgroup.
Chemotherapy, which is fundamental for the treatment of metastatic breast cancer, is reported to rarely cure due to the presence of minimal residual disease that has spread to other organs. A pilot study was designed to test whether vitamin A (as retinyl palmitate) in combination with interferon and tamoxifen could improve overall survival in metastatic breast cancer patients.109 The results showed that the combination was feasible and showed activity in metastatic breast cancer with an acceptable level of toxicity.
Preclinical models suggest that synthetic retinoids can inhibit mammary carcinogenesis.110 In a recent review of clinical trials with synthetic retinoids for breast cancer chemo prevention it was reported that a phase III breast cancer prevention trial, investigating fenretinide (a synthetic retinoid derivative of vitamin A), showed a durable trend to a reduction of second breast malignancies in pre-menopausal women. This pattern was associated with a favourable modulation of circulating IGF-I and its main binding protein IGFBP-3, which have been associated with breast cancer risk in pre-menopausal women in different prospective studies.111 Moreover, a recent study showed that fenretinide positively balanced the metabolic profile in overweight pre-menopausal women at high risk for breast cancer, and this was postulated to perhaps favourably affect breast cancer risk.112
All trans retinoic acid (ATRA) (also known as Tretinoin) is the acid form of vitamin A. A phase II trial employed all trans retinoic acid so as to evaluate its tumour cytoreduction in patients with metastatic breast cancer and to characterise the initial pharmacokinetics of the compound.113 The study concluded that ATRA did not have any significant activity in patients with hormone refractory metastatic breast cancer.
A phase I–phase II combination clinical trial with tamoxifen and ATRA in patients with advanced breast cancer investigated their additive antitumor effects.114 The study showed that declines in serum IGF-I concentrations observed in patients treated with tamoxifen and ATRA were similar to those observed in patients treated with tamoxifen alone. Additional studies are warranted to further investigate these data.
Lycopene
The epidemiologic literature regarding intake of tomatoes and tomato-based products and blood lycopene (a compound derived predominantly from tomatoes) level in relation to the risk of various cancers was reviewed. The outcome suggested strongly that there was a consistently lower risk of cancer for a variety of anatomic sites (including breast) that was associated with higher consumption of tomatoes and tomato-based products adding further support for current dietary recommendations to increase fruit and vegetable consumptions.115
A recent review concluded that the emerging area of health-derived benefits from food sources such as lycopene requires additional investigations into its effects on breast cancer.116
Integrative management of malignant breast disease
Lifestyle
Breast cancer can spread insidiously. The prevalence in the US during the years 2000–2004 in women aged 20–24 years had the lowest breast cancer incidence rate of 1.4 cases per 100 000 women, and women aged 75–79 years had the highest incidence rate of 464.8 cases per 100 000. The decrease in age-specific incidence rates that occurs in women aged 80 years and older may reflect lower rates of screening, the detection of cancers by mammography before age 80, and incomplete detection.117
An early investigation of approximately 25 000 women diagnosed with breast cancers reported that at diagnosis, 5–15% of patients had metastatic disease and almost 40% had regional spread of the disease.118
Promotion of behaviour patterns that optimise energy balance (i.e. weight control and increasing physical activity) may be viable options for the prevention of breast cancer. Researchers from the US and Peoples Republic of China (PRC) have evaluated the hypothesis that a pattern of behavioural exposures indicating positive energy balance (i.e. less physical activity/sport activity, high BMI, or high energy food intake) would be associated with an increased risk for breast cancer in the Shanghai Breast Cancer Study.119 This population-based study comprised 1459 incident breast cancer cases and 1556 age frequency-matched controls. Participants completed in-person interviews that collected information on breast cancer risk factors, usual dietary intake and physical activity in adulthood. Anthropometric indices were also measured. The study concluded that lack of physical activity/sport activity, low occupational activity, and high BMI were all individually associated with an increased risk for breast cancer (odds ratios [OR] 1.49 to 1.86).
A recent study has summarised that lifestyle changes including continuous or intermittent energy restriction and/or physical activity may be significantly beneficial for preventing breast cancer.120
Mind–body medicine
Cancer is a profoundly stressful experience. A cancer diagnosis is full of trepidation by most people because of its life-threatening implications and the potentially serious side-effects of the treatments. Hence, mind–body therapies have become more popular within cancer populations as methods to treat physical and psychiatric symptoms in conjunction with conventional allopathic care. Interventions such as support groups, educational programs, guided imagery, and expressive writing have been studied and are now frequently incorporated into plans of care for all types of cancer patients.121, 122, 123
Psychotherapeutic and social support interventions provide emotional and other psychological benefits to cancer patients.124 Group, individual and family interventions have been shown to reduce depression and anxiety, improve coping and mobilise social support.125, 126 However, what is more controversial are findings that psychosocial interventions may affect the course of the disease as well as the adjustment to it. Most people are ready to accept that changes in physical status influence cognition and affect.127 In the context of a holistic approach to health that includes the concept of unity of mind and body, it makes sense that intervention at a mental level might have physical consequences.128
Research by a number of investigators has reported that patients who underwent psychological intervention lived longer than the national average.129–132 Some researchers have analysed the psychological attributes associated with patients who survive what is thought to be terminal cancer. Roud133 noted that all long-term survivors believed that there was a direct relationship between the outcomes experienced and their psychological states. They remained confident that they would not die, and felt that these positive expectations were critical to the healing process. They assumed responsibility for all aspects of their lives, including recovery and established relationships with physicians described as trusting, meaningful, and healing.
The key components of effective interventions appear to be:
These interventions help cancer patients prepare for the worst but hope for the best. All have the goal of living better, and improve prognosis.
Mindfulness meditation
Mindfulness meditation is a form of mind–body therapy that is gaining credibility and interest for use in oncology patients.135 It has been reported that the primary emphasis of mindfulness meditation is experiencing life fully and being in touch with the full range of human emotions and sensory experiences. Rather than a method to control or change unpleasant or unwanted emotions, thoughts, or sensations, mindfulness meditation is a way of being engaged in the complete experience of what is happening in the present moment without getting entangled in reflections about previous experiences or an anticipated future.136, 137 Mindfulness meditation will often elicit relaxation, and as a result, offers individuals a way to alleviate suffering that often accompanies pain or emotional discomfort.138
Mindfulness Based Stress Reduction (MBSR)
MBSR is a well-defined, systematic, educational, patient-focused intervention with formal training in mindfulness meditation and its applications in everyday life, which includes managing physical and emotional pain for cancer patients.136
A recent study demonstrated that MBSR is a significantly effective program that is feasible for women recently diagnosed with early stage breast cancer and the results provided preliminary evidence for beneficial effects of MBSR on immune function, quality of life and coping.139 A further study utilising MBSR to investigate a 1-year pre-post intervention follow-up of psychological, immune, endocrine and blood pressure outcomes demonstrated that MBSR program participation was associated with enhanced quality of life and decreased stress symptoms, altered cortisol and immune patterns.140 These results were consistent with less stress and mood disturbances, and decreased blood pressure. The pilot data represented a preliminary investigation of the longer-term relationships between MBSR program participation and a range of potentially important biomarkers in patients with breast cancer.
Overall recent reviews conclude that from all the current available scientific evidence, MBSR may be a potentially beneficial intervention.141, 142 Moreover, a recent clinician’s guide to MBSR concluded that it was a safe, effective, integrative approach for reducing stress. Also both patients and health care providers experiencing stress or stress-related symptoms may benefit from MBSR programs.143 MBSR interventions can be safely and effectively used in a variety of patient populations.
Cognitive behaviour therapy (CBT)
CBT was found to be helpful for survivors of breast cancer who reported cognitive impairment after chemotherapy in a single-arm pilot study.144 Ferguson et. al. reported that a specialised intervention using CBT principles called ‘memory and attention adaptation training’ was delivered to 29 survivors of breast cancer. The study concluded that participants reported high treatment satisfaction and rated the memory and attention adaptation training as helpful in improving ability to compensate for memory problems. Given these results, the CBT treatment appears to be a feasible and practical cognitive behaviour program that necessitates continued evaluation among cancer survivors who experience persistent cognitive dysfunction.
Few studies have examined the experience of cognitive impairment and how it affects day-to-day life. A small interview-based study with 10 survivors of breast cancer who reported cognitive impairment after chemotherapy showed that the women who reported the most disruption from cognitive impairment were those with high-stress occupations and coping with professional and family commitments.145
A recent Cochrane review that assessed the effects of psychological interventions (educational, individual cognitive behavioural, psychotherapeutic, or group support) on psychological and survival outcomes for women with metastatic breast cancer reported that there was insufficient evidence to advocate that group psychological therapies be recommended to women with metastatic breast cancer.146 However, this review did not analyse the results of other studies that showed benefit for psychological therapies.147
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


