Breast and Female Reproductive System
Valerie A. Fitzhugh
Joann Habermann
Debra S. Heller
▪ Questions and Answers
1. A 54-year-old multiparous woman presents with a painless, poorly defined subareolar mass, accompanied by thick, white nipple secretions. The histology of the lesion is shown (Fig. 12.1). Which of the following is TRUE of the lesion?
a. It is associated with cigarette smoking.
b. The lesion is characterized by a dilatation of ducts, inspissation of breast secretions, and a marked periductal and interstitial chronic granulomatous inflammatory reaction.
c. The periductal and interductal inflammation is manifested by heavy infiltrates of neutrophils.
d. The mass is an intraductal papilloma.
e. This lesion is not usually mistaken as carcinoma clinically.
View Answer
1. b. The lesion depicted in the image is mammary duct ectasia. The history is classic. The lesion is characterized by a dilatation of ducts, inspissation of breast secretions, and a marked periductal and interstitial chronic granulomatous inflammatory reaction. Smoking is associated with periductal mastitis. The infiltrate associated with periductal mastitis consists of lymphocytes and macrophages. Intraductal papillomas do not present with thick secretions. Duct ectasia is of clinical significance because it can be confused with carcinoma by palpation and on mammographic examination.
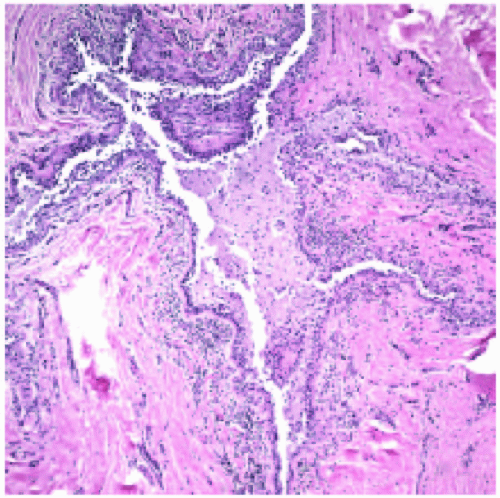 Figure 12.1 |
2. All of the following findings are associated with fibrocystic changes of the breast EXCEPT:
a. Cysts
b. Apocrine metaplasia
c. Fibrosis
d. Atypical ductal hyperplasia
e. Adenosis
View Answer
2. d. The histologic findings in fibrocystic breast changes are cyst formation, often with apocrine metaplasia, fibrosis, usually secondary to cyst rupture, and adenosis. These are all forms of nonproliferative breast changes. Atypical ductal hyperplasia is a form of proliferative breast disease and is not a component of fibrocystic changes.
3. Which set of findings is most commonly seen in proliferative breast disease without atypia?
a. Moderate to florid epithelial hyperplasia, apocrine metaplasia, sclerosing adenosis, papilloma
b. Atypical lobular hyperplasia, apocrine metaplasia, radial scar, fibroadenoma with complex features
c. Moderate or florid hyperplasia, sclerosing adenosis, papilloma, radial scar
d. Duct ectasia, cysts, radial scar, sclerosing adenosis
e. Fibroadenoma without complex features, radial scar, papilloma, atypical lobular hyperplasia
View Answer
3. c. Changes of the breast in proliferative disease without atypia include moderate to florid hyperplasia, sclerosing adenosis, papilloma, complex sclerosing lesion or radial scar, and fibroadenoma with complex features. Nonproliferative (fibrocystic) breast changes include duct ectasia, apocrine metaplasia, cysts, adenosis, and fibroadenoma without complex features, as well as fibroadenomatoid change. Changes of the breast in proliferative disease with atypia include atypical ductal and lobular hyperplasia.
4. The most common risk factors for breast cancer include all of the following EXCEPT:
a. Age
b. Age at menarche
c. Race
d. Age at first live birth
e. Second-degree relatives with breast cancer
View Answer
4. e. The most common risk factors for the development of breast carcinoma as identified by epidemiologic studies include age, age at menarche, age at first live birth, first-degree relatives with breast cancer, history of breast biopsies, and race. A history of second-degree relatives with breast cancer is not identified as a risk factor. Additional recognized risk factors include estrogen exposure, radiation exposure, carcinoma of the contralateral breast or endometrium, geographic influence, diet, obesity, exercise, breastfeeding, and environmental toxins.
5. Which of the following is true regarding to the hereditary breast cancer gene BRCA1?
a. The gene is located on chromosome 13q12.3.
b. It functions as an anti-apoptotic factor.
c. Patients have late onset of breast carcinoma.
d. Other locations where carcinoma can occur include ovary, colon, and pancreas.
e. There is a lower incidence of medullary carcinoma, poorly differentiated carcinomas, ER and PR negativity, and HER-2/neu negativity.
View Answer
5. d. The BRCA1 is located on chromosome 17q21. It is a tumor suppressor gene, not an antiapoptotic factor. Patients tend to have an early onset of breast carcinoma, often in their 40s and 50s. There is a risk of other carcinomas in the ovary, colon, and pancreas. These patients have a greater incidence of medullary carcinoma of the breast, poorly differentiated carcinomas, ER and PR negativity, and Her-2/neu negativity.
6. A 66-year-old woman has a mammographic density and presents with the lesion shown (Fig. 12.2). Which of the following is true of this lesion?
a. It is characterized by solid sheets of low-grade nuclei and central necrosis.
b. The necrotic cell membranes commonly calcify and are detected on mammography as clusters or linear and branching microcalcifications.
c. Periductal concentric fibrosis and chronic inflammation are uncommon.
d. Extensive lesions are never palpable as an area of vague nodularity.
e. It is one of the subtypes of invasive carcinoma.
View Answer
6. b. The lesion depicted here is comedocarcinoma. It is characterized by solid sheets of pleomorphic cells with high-grade nuclei and central necrosis. The necrotic cell membranes do indeed calcify and are detected on mammography as clusters or linear and branching microcalcifications. Periductal concentric fibrosis and chronic inflammation are common. Extensive lesions may be palpable as a vague nodule. It is one of the subtypes of ductal carcinoma in situ (DCIS).
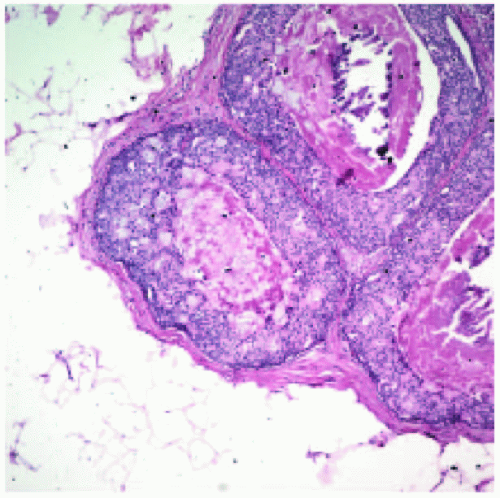 Figure 12.2 |
7. Which of the following is true regarding the molecular characteristics of lobular carcinoma?
a. Most show a loss of chromosome 16q22.1 that includes a cluster of at least eight genes responsible for cell-cell adhesion, including e-cadherin and β-catenin.
b. HER-2/neu overexpression is extremely common in well to moderately differentiated types.
c. Poorly differentiated tumors have a tendency to overexpress hormone receptors.
d. Tumors with better differentiation tend to show aneuploidy on DNA ploidy analysis.
e. The E-cadherin on the opposite chromosome (i.e., the one that does not show loss) is upregulated by mutations.
View Answer
7. a. Most invasive lobular carcinomas show a loss of chromosome 16q22.1 that includes a cluster of at least eight genes responsible for cell-cell adhesion, including E-cadherin and β-catenin. Well to moderately differ – entiated tumors are diploid with increased hormone receptor expression and decreased HER-2/neu expression. Poorly differentiated tumors tend to be aneuploid with decreased hormone receptor expression and increased HER-2/neu expression. The E-cadherin on the opposite chromosome (i.e., the one that does not show loss) is inactivated by mutations, not upregulated.
8. Which of the following statements is true regarding fibroadenomas?
a. The lesion is generally benign and occurs in patients between 45 and 60 years of age.
b. The lesion “giant fibroadenoma” is most common in white women in the adolescent years.
c. The stroma of fibroadenoma is usually made up of CD34 positive fibroblasts and scattered factor XIIIa positive dendrophages.
d. The lesions tend to increase in size both during pregnancy and as the patient ages.
e. In cases with apocrine metaplasia, the metaplastic cells are negative for GCDFP-15.
View Answer
8. c. Fibroadenomas are the most common benign breast neoplasm in women from ages 20 to 35. The variant giant fibroadenoma shows a racial predilection for black females in the adolescent years. The stroma of fibroadenomas includes CD34 positive fibroblasts and Factor XIIIa positive dendrophages. While these lesions are seen to increase in size during pregnancy, they decrease in size as the patient ages, leading to increased hyalinization and decreased stromal elements. Fifteen percent of fibroadenomas show apocrine metaplasia, and the metaplastic cells stain positively for GCDFP-15.
9. All of the following statements regarding the evolution of ductal carcinoma in situ (DCIS) into invasive ductal carcinoma are true EXCEPT:
a. The transformation to an invasive phenotype does not occur in all cases.
b. If the transformation from DCIS to invasive ductal carcinoma does occur, it can take years to decades.
c. The risk of transformation is lower in cases of comedocarcinoma than in noncomedo types of DCIS.
d. The microscopic type of DCIS correlates closely to the invasive type seen later.
e. Some invasive ductal carcinomas go through a very short in situ stage before becoming invasive, leading to difficulty in detecting them clinically before invasion.
View Answer
9. c. While ductal carcinoma in situ (DCIS) is accepted as a precursor lesion to invasive ductal carcinoma, progression to an invasive type does not occur in all cases. In most cases, the process of transformation may take years to decades, but in some patients, the interval to transformation is much shorter. There is a definite relation between the microscopic type of DCIS and the invasive component seen later. The risk of transformation in comedocarcinoma is much higher than in cases of noncomedo DCIS.
10. The lesion shown was excised from the breast of a 58-year-old woman (Fig. 12.3). Which of the following immunohistochemical markers will be most helpful in establishing the diagnosis?
a. Cytokeratin AE1/AE3
b. Epithelial membrane antigen (EMA)
c. Gross cystic disease fluid protein-15 (GCDFP-15)
d. E-cadherin
e. Lactalbumin
View Answer
10. d. The lesion depicted in this figure is invasive lobular carcinoma, which is highlighted by tumor cells in a single-file pattern and a minimally desmoplastic stroma in many cases. Cytokeratin AE1/AE3, EMA, GCDFP-15, and lactalbumin are common to many lesions of the breast. E-cadherin distinguishes lobular carcinoma from other processes in the breast because of its negative staining pattern. Most cases of lobular carcinoma show a loss of chromosome 16q22.1, resulting in a loss of the E-cadherin gene.
 Figure 12.3 |
11. Which of the following characteristics is necessary for the pathologic diagnosis of inflammatory carcinoma of the breast?
a. There must be clinical inflammation and edema of the skin of the breast.
b. Dermal lymphatic invasion must be seen histologically.
c. Calcifications must be identified radiographically.
d. Large clear cells must be seen in the epithelial layers of the breast.
e. The lesion of the nipple of the breast must be differentiated from eczema.
View Answer
11. b. Inflammatory carcinoma of the breast was originally a clinical diagnosis (i.e., the entire breast was reddened and warm with edema). Histologic studies of some of the cases revealed an undifferentiated carcinoma invading the dermal lymphatics of the breast. It was found that some cases showed dermal lymphatic invasion without overt clinical symptoms. Calcifications may be seen, but do not contribute to the pathologic diagnosis. Large clear cells in the epidermis are a finding in Paget disease of the breast, as are eczematous type changes of the nipple.
12. Which of the following immunohistochemical stains is most useful in the differential diagnosis of Paget disease of the breast and melanoma?
a. Carcinoembryonic antigen (CEA)
b. Cytokeratin 7
c. HMB-45
d. Epithelial membrane antigen (EMA)
e. Cytokeratin AE1/AE3
View Answer
12. c. In Paget disease of the breast, one may see intracytoplasmic melanin granules in the cytoplasm of the tumor cells. The granules have most likely been transferred from neighboring melanocytes by the process of cytocrinia, in which the tumor cells have imbibed melanin. In this case, and to avoid an erroneous diagnosis of melanoma, the HMB-45 immunostain is most useful, as it will be positive in melanoma and negative in Paget disease of the breast.
13. Which of the following is true in the comparison of phyllodes tumor and fibroadenoma?
a. Phyllodes tumors and fibroadenomas do not fall within the same age group.
b. Fibroadenomas and phyllodes tumors are always easily distinguishable.
c. Phyllodes tumors tend to show a dense stromal hypercellularity.
d. The mitotic count is unimportant when attempting to determine whether the neoplasm is a fibroadenoma or a phyllodes tumor.
e. Unlike fibroadenomas, phyllodes tumors are not diagnosed at small size.
View Answer
13. c. Phyllodes tumors and fibroadenomas are both fibroepithelial lesions of the breast. Fibroadenomas are more common before the age of 30, whereas phyllodes occur in the 40s. The stroma is extremely important when trying to decide between a phyllodes tumor and a fibroadenoma. Phyllodes tumors are distinguished from fibroadenomas on the basis of cellularity, mitoses, stromal overgrowth, nuclear pleomorphism, and infiltrative borders. Malignant phyllodes tumors show a dense stromal cellularity with mitoses, while it is more common to see a loose connective tissue stroma without mitotic activity in fibroadenomas. phyllodes tumors are often diagnosed at smaller sizes because of increased awareness of breast disease, much like fibroadenomas.
14. A 58-year-old woman presents with a wellcircumscribed breast mass. The histology is demonstrated (Fig. 12.4). Which of the following is true of this lesion?
a. Grossly, foci of hemorrhage are infrequent.
b. This tumor has weak immunoreactivity for MUC2 and increased immunoreactivity for MUC1 when compared with ductal carcinoma not otherwise specified.
c. The mucin in this lesion is extracellular and may be of acid or neutral type.
d. Of these lesions, 75% show features consistent with endocrine differentiation.
e. Grossly, these lesions are poorly defined.
View Answer
14. c. The lesion in the figure represents mucinous carcinoma. It is characterized histologically by small clusters of tumor cells floating in large pools of mucin as seen here. Foci of hemorrhage within these tumors are frequently seen. The tumor has strong cytoplasmic reactivity for MUC2 and decreased reactivity for MUC1 when compared with ductal carcinoma NOS. One quarter to one half of these tumors show endocrine differentiation consisting of argyrophilia, neuron specific enolase positivity, and dense core granules on electron microscopy. The mucin in the tumor is almost entirely extracellular and it may be of acid or neutral type. Grossly, these lesions tend to have sharply defined borders.
15. A 51-year-old woman presents with a 1-cm breast mass. The lesion was excised and the histology is shown. (Fig. 12.5) Which of the following is the best answer?
a. The lesion can be easily differentiated from radial scar and microglandular adenosis on microscopic examination.
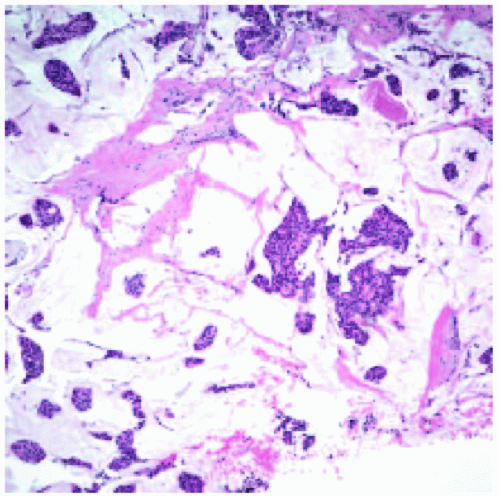 Figure 12.4 |
b. These lesions can be characterized by angulated glands, apical blebbing, and luminal calcifications.
c. It is unusual for these tumors to be underdiagnosed as a benign process on fine needle aspiration biopsy.
d. Metastases to axillary lymph nodes occur in 50% of cases and the prognosis is poor.
e. This diagnosis is common, accounting for 35% to 40% of breast carcinoma diagnoses.
View Answer
15. a. The tumor in this image is an example of tubular carcinoma. The angulated shape of the glands and apical snouts are characteristic features of this lesion. Calcifications were noted elsewhere in the lesion. Mitotic figures are absent in these lesions and nuclear pleomorphism is scant. Because of the marked degree of cellular differentiation in these lesions, it is not at all unusual for them to be underdiagnosed as benign. Metastases to the axillary lymph nodes occur in only 10% of cases and the prognosis is excellent. Because of the well-differentiated nature of this lesion, radial scar and microglandular adenosis are important differential diagnostic considerations and are sometimes difficult to differentiate from tubular carcinoma. The diagnosis is relatively uncommon, accounting for a frequency of 1% to 3% in clinical practice.
16. Which of the following statements about HER-2/neu is true?
a. HER-2/neu is an oncogene that encodes a transmembrane glycoprotein with tyrosine kinase activity known as p185, which belongs to the family of epidermal growth factor receptors.
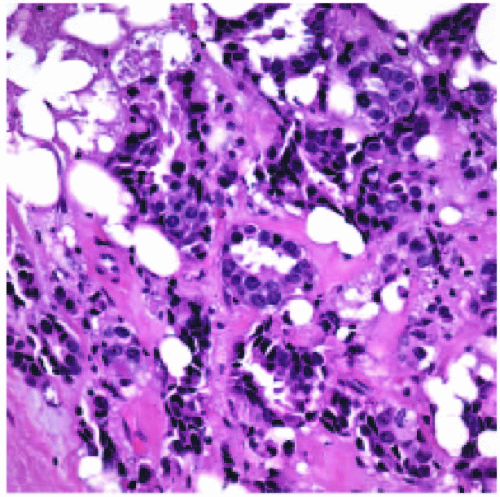 Figure 12.5 |
b. Its overexpression can be measured by immunohistochemistry but not by fluorescence in situ hybridization (FISH).
c. HER-2/neu negativity is an indication to treat a patient with trastuzumab.
d. Overexpression of HER-2/neu is a very good predictor of response to chemotherapy and overall survival.
e. There is no improvement in patient response when treatment for HER-2/neu therapy is combined with conventional chemotherapy.
View Answer
16. a. HER2/neu is an oncogene that encodes a transmembrane glycoprotein with tyrosine kinase activity known as p185, which belongs to the family of epidermal growth factor receptors. Its overexpression can be measured by immunohistochemistry and FISH. The performance of FISH is recommended for immunoreactivity graded 1+ and 2+. Overexpression (or positivity) of HER2/neu is seen in more aggressive tumors is an indication to treat patients with trastuzumab (Herceptin), which specifically targets HER2 receptors. Several centers have reported improvement in patient response when HER-2/neu therapy is combined with conventional chemotherapy.
17. All of the following lesions can present as a breast mass EXCEPT:
a. Sarcoidosis
b. Coccidiomycosis
c. Silicone reaction
d. Blunt duct adenosis
e. Breast abscess
View Answer
17. d. Blunt duct adenosis is a histologic diagnosis and a clinically evident mass is not usually associated. Sarcoidosis, coccidiomycosis, breast abscess, and silicone reaction can all cause single or multiple breast masses in patients.
18. A 46-year-old woman has a lesion in association with an intraductal papilloma. The histology is shown (Fig. 12.6). Which of the following is true of this lesion?
a. This lesion is only seen in association with intraductal papilloma.
b. This lesion may also be seen in salivary gland tumors.
c. Carcinoma is not seen in association with these lesions in the breast.
d. Ultrastructurally, collagen is not seen.
e. These lesions are positive for Alcian blue.
View Answer
18. b. The histology represented here is that of collagenous spherulosis. It is characterized by the presence of intraluminal clusters of generally eosinophilic but sometimes basophilic collagen-rich spherules that seem to arise within the spaces between the epithelial and myoepithelial cells. The lesion can be seen in association with intraductal papilloma and sclerosing adenosis. Exceptionally, foci of lobular carcinoma in situ can involve this lesion. Collagen is seen ultrastructurally in association with basement membrane material and mineral deposition. Collagenous spherulosis can be seen in association with salivary gland tumors. Because this lesion does not contain any type of mucin, it would not be positive for Alcian blue.
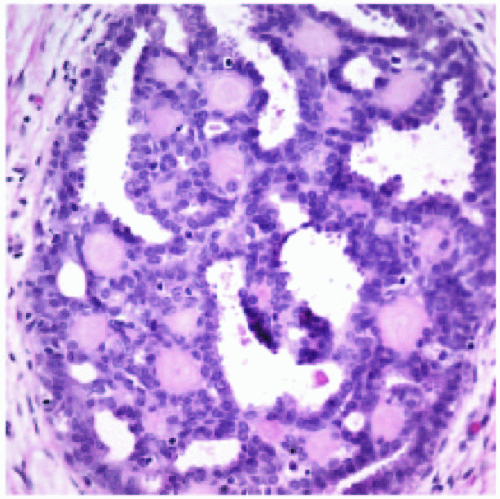 Figure 12.6 |
19. Which of the following pairs of information correctly stratifies the risk of carcinoma associated with breast hyperplasia?
a. No or mild hyperplasia: 3 to 4 times the risk for subsequent invasive carcinoma.
b. Moderate or florid hyperplasia: 1.5 to 2 times the risk for subsequent invasive carcinoma.
c. Atypical ductal or lobular hyperplasia: 7 times the risk for subsequent invasive carcinoma.
d. Ductal or lobular carcinoma in situ: 13 to 15 times the risk for subsequent invasive carcinoma.
View Answer
19. b. A group convened by the College of American Pathologists recommended grouping patients with fibrocystic lesions in the following categories:
I. No or mild hyperplasia: no increased risk for subsequent invasive carcinoma.
II. Moderate or florid hyperplasia: 1.5 to 2 times the risk.
III. Atypical ductal or lobular hyperplasia: 5 times the risk.
IV. Ductal or lobular carcinoma in situ: 8 to 10 times the risk. (This fourth category, although not fibrocystic breast disease, was added by the group for the sake of completeness.)
20. Each of the following tumors is a subtype of ductal carcinoma EXCEPT:
a. Tubular carcinoma
b. Mucinous carcinoma
c. Histiocytoid carcinoma
d. Cribriform carcinoma
e. Metaplastic carcinoma
View Answer
20. c. Histiocytoid carcinoma is a cytologic variant of invasive lobular carcinoma and therefore does not belong to the invasive ductal carcinoma subgroup. Tubular, mucinous, metaplastic, and cribriform carcinomas are all distinct subtypes of invasive ductal carcinoma.
21. A 66-year-old woman is diagnosed with the lesion shown in the photomicrograph (Fig. 12.7).Which of the following is true about this disease?
a. This invasive tumor does not exhibit the pattern of growth of a classical breast carcinoma.
b. This lesion frequently shows apocrine differentiation, signet ring morphology and nuclear pleomorphism.
c. E-cadherin immunostaining is frequently positive.
d. Expression of p53 and HER-2/neu is low.
View Answer
21. b. This is an example of pleomorphic lobular carcinoma. It has the pattern of growth of a classical invasive lobular carcinoma complete with the single cell file pattern of growth but exhibits a marked degree of nuclear pleomorphism and abundant cytoplasm. It frequently shows apocrine metaplasia and focal signet ring morphology. Expression of p53 and HER2/neu is very high. Lack of E-cadherin staining is in keeping with the lobular nature of the tumor.
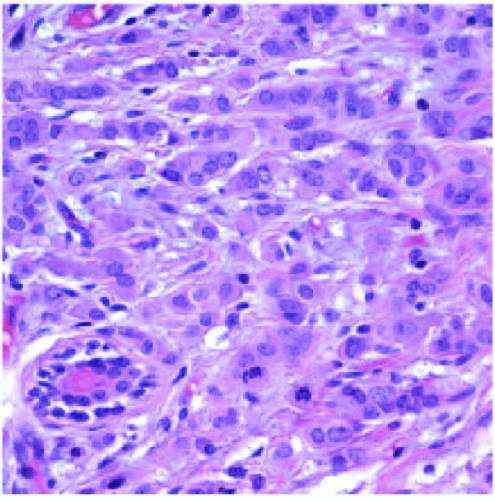 Figure 12.7 |
22. Which of the following is true regarding angiosarcoma of the breast?
a. It is not seen following an axillary dissection.
b. Freely anastomosing vascular channels with malignant endothelial cells are rarely seen.
c. The tumor is thought to be derived from lymph vessels rather than blood vessels.
d. The differential diagnosis includes metaplastic carcinoma, acantholytic variant of squamous cell carcinoma, and pseudoangiomatous stromal hyperplasia (PASH).
e. Postradiation angiosarcoma is less common than angiosarcoma de novo.
View Answer
22. d. Angiosarcoma can occur secondary to lymphedema following axillary dissection. Microscopically, the diagnostic areas are characterized by freely anastomosing vascular channels lined with atypical cells. The tumor is thought to arise from blood vessels, not lymph vessels. The differential diagnosis includes metaplastic carcinoma, the acantholytic variant of squamous cell carcinoma, and pseudoangiomatous stromal hyperplasia. Radiation-induced angiosarcomas are actually more common than de novo angiosarcomas and can occur anywhere from 2.5 to 10 years after radiation is given.
23. A 27-year-old woman presents with a breast mass that is excised. The histology is demonstrated (Fig. 12.8). Which of the following statements about this lesion is most correct?
a. It grossly simulates the appearance of invasive carcinoma.
b. Tumors are on average 10 cm or more in greatest dimension.
c. The tumor is aggressive and excision should be wide.
d. The cytoplasm is negative for periodic acid Schiff (PAS) stain.
e. The overwhelming majority of these cases are malignant.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


