FIGURE 11-1 Twelve-lead ECG after cardioversion, demonstrating manifest preexcitation with deeply negative delta waves in leads II, III, and aVF.
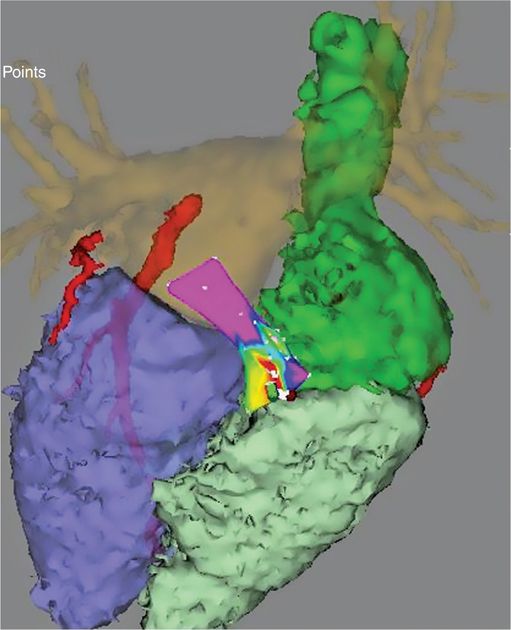
FIGURE 11-2 Site of successful epicardial mapping and ablation. This shows a fusion of electroanatomic mapping from the epicardial space (with colors indicating timing of earliest preexcited ventricular electrogram) with a previously acquired CT scan of the heart. The left and right atria and ventricles can be seen in the CT image, as well as the relevant portions of the right and left circumflex coronary arteries, which are adjacent to the ablation site.
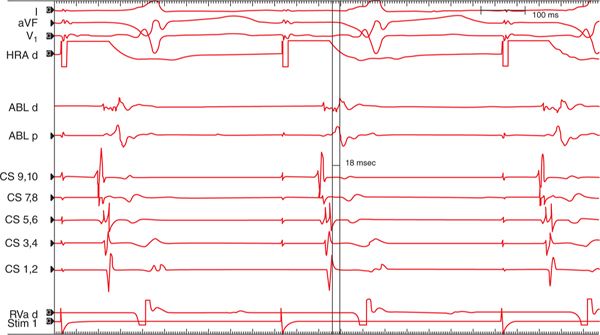
FIGURE 11-3 Surface and intracardiac electrograms from the successful ablation site. Mapping was performed during high right atrial (HRA) pacing. Tracings are shown from surface leads I, V1, and aVF, as well as HRA, ablation (ABL) proximal and distal electrograms, coronary sinus (CS) proximal (9,10) to distal (1,2), and right ventricular apex (RVa). The earliest accessory pathway (AP) electrograms are noted 18 ms before the onset of the delta wave visualized on the surface leads.

FIGURE 11-4 Loss of preexcitation during ablation. These electrograms (same annotation as Figure 11-3) were obtained during ablation at the same site as Figure 11-3. The first 2 beats show preexcitation on the surface leads, which is no longer evident on the 3rd and subsequent beats. In addition, the short delay between the local atrial and ventricular electrograms in the preexcited beats noted on the ablation catheter lengthens with loss of preexcitation. Loss of preexcitation was noted after 6.5 seconds of ablation at this site and was durable after completion of ablation and administration of IV adenosine.
EPIDEMIOLOGY AND PATHOPHYSIOLOGY
Manifest preexcitation is evident in approximately 0.1% to 0.3% of ECGs,2 although this underestimates the true prevalence of AP conduction, as many APs are concealed, either due to AV nodal conduction preceding AP conduction or due to lack of anterograde AP conduction. Classic APs result from electrically excitable fibers (bundles of Kent) which pass through the fibrous AV ring, although other types of APs (ie, atriofascicular pathways) have also been extensively described in the literature.3
The initial interventional approaches to patients with symptomatic Wolff-Parkinson-White (WPW) syndrome involved cardiac surgical incisions in the region of the AP.4 Because these incisions were transmural, the exact intramural location of the AP (endocardial, midmyocardial, or epicardial) was generally not relevant for clinical success in most cases. This changed with the advent of catheter ablation,5 however, as current ablation catheters may not always create transmural lesions, particularly in regions of thick myocardium, such as the AV ring (particularly relevant to AP ablation) and the ventricular septum and left ventricle (relevant to ventricular tachycardia ablation).
If microscopic studies could be performed on all APs, it would be possible to anatomically define the course of each AP, and endocardial/epicardial location could be precisely determined. Because this is obviously not possible in patients, the location of a given AP is typically defined based on activation mapping of the region of earliest atrial and/or ventricular preexcitation and AP potentials, and particularly by success (or lack of success) of ablation at a given site. Epicardial APs are typically defined as those which require epicardial access for successful ablation, as well as APs which map to and/or are successfully ablated from the coronary sinus (CS) and its tributaries, which is an epicardial structure. This is thus a functional rather than a true anatomic classification of endocardial/epicardial location of APs, and it should be noted that pericardial mapping (other than mapping within the CS) is rarely performed for a given AP unless ablation from an endocardial approach is unsuccessful. APs requiring pericardial access for successful ablation have generally been reported as single cases or small case series, and so it is currently difficult to estimate their true incidence.1,6–9 In comparison, APs which have been successfully ablated from within the CS or its tributaries have been described with much greater frequency.10
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


