This chapter is an overview of current principles and methods for assessment and management of acquired aphasia in adults in post-acute clinical settings. Current evidence-based approaches to aphasia treatment and management are emphasized, as well as the practical clinical decisions involved in designing treatment for individuals and stroke survivor groups. (For a discussion of speech-language pathology in acute care settings, see Chapter 15; for more information on the differential diagnosis of language disturbance, see Chapter 4.)
This chapter addresses several areas of knowledge identified by the American Speech-Language-Hearing Association (ASHA) as standard competencies for the Certificate of Clinical Competence in Speech-Language Pathology, effective in 2014. 1 Specifically, this chapter relays knowledge in the areas of basic human communication processes (Standard IV-B), communication disorders and differences (Standard IV-C), and the principles and methods of assessment and intervention for people with communication disorders (Standard IV-D).
The trained speech-language pathologist (SLP) is prepared to assume the following roles in providing optimal patient care for the person with aphasia (PWA): (1) communication partner, (2) diagnostician, (3) therapist, (4) researcher, and (5) educator/advocate. The SLP is particularly aware of communication cues and strategies that may benefit each PWA and is able to educate other communication partners and to advocate for the PWA in managing the effects of aphasia on life participation. As a diagnostician and therapist, the SLP must link neurologic, cognitive, linguistic, and functional areas of the PWA’s condition with evidence-based approaches to intervention. Finally, there is no necessary division between clinician and researcher, as the SLP clinician evaluates the effectiveness of one intervention approach over another within and across PWAs.
5.1 Assessment of Aphasia
Adults with acquired aphasia have impaired language skills secondary to neurologic injury or disease affecting the central nervous system (CNS), often a stroke in the left hemisphere perisylvian region. Normal language can break down in varied and complex ways, yet similar patterns among PWAs provide clues to the underlying source of impairment and to promising treatment approaches. The goal of comprehensive aphasia assessment is to identify intact language abilities as well as cognitive-linguistic impairments.
The World Health Organization’s International Classification of Functioning, Disability, and Health 2 (ICF) is a framework for assessing and defining patient needs that may be addressed specifically in rehabilitation. The ICF includes codes defining language abilities. It also includes activity and participation codes that allow the clinician to report the range of effects that aphasia has on a PWA’s life, and potential improvements in life participation following aphasia treatment. These life participation concepts have been included in ASHA’s revised Scope of Practice for Speech-Language Pathology 3 document, and speech-language pathology is described as encompassing health conditions (i.e., body functions and structures; activity and life participation) and contextual factors (i.e., environmental and personal factors) that influence an individual’s functioning and disability. Among other factors the SLP considers are a person’s background and culture and how they may influence the person’s reaction to a communication disorder.
5.1.1 Aphasia Subtypes and Evolution of Aphasia
The traditional subtypes of aphasia are differentiated by performance in fluency, auditory comprehension, and repetition. Impaired naming (i.e., anomia) is common to all aphasia subtypes. These language skills can be screened using commercially available aphasia tests such as the Boston Diagnostic Aphasia Examination 4 (BDAE), the Western Aphasia Battery-Revised 5 (WAB-R), and the Boston Naming Test 6 (BNT). Within subtype, individuals will differ in level of severity and in more detailed language features distinguishable by using error analysis or measures like the Psycholinguistic Assessments of Language Processing in Aphasia 7 (PALPA).
Nonfluent aphasia is defined by a constellation of symptoms involving reduced phrase length, quantity of output, speech rate, articulatory agility, grammatical complexity, and thematic elaboration. 8 Aphasia subtypes defined as having poor auditory comprehension are marked by impaired understanding of single words and sentences, in the more severe cases even affecting high-frequency concrete words. When auditory comprehension is categorized as good overall, auditory comprehension still may be reduced for low-frequency words, abstract words, or specific types of sentences.
An individual’s aphasia often evolves from one traditional subtype to another. 9 In ▶ Table 5.1, the aphasia subtypes are listed to allow comparison of how each type would be reclassified based on evolution of fluency, auditory comprehension, and repetition. For example, global aphasia would evolve to Broca’s aphasia if auditory comprehension improved significantly. If only fluency improved, global aphasia would evolve to Wernicke’s aphasia. Broca’s aphasia could evolve to anomic aphasia if fluency and repetition both improved. Anomic aphasia may persist despite the evolution of other aphasia symptoms. 9
Nonfluent Aphasias Auditory Comprehension | Fluent Aphasias Auditory Comprehension | |||
Poor | Good | Poor | Good | |
Repetition |
| |||
Poor | Global | Broca’s | Wernicke’s | Conduction |
Good | TC Mixed | TC Motor | TC Sensory | Anomic |
TC= Transcortical | ||||
5.1.2 Cognitive-Linguistic Assessment of Aphasia
Cognitive-linguistic impairments that underlie reduced language skill in aphasia can be linked to specific sources of disruption within the normal language system. Normal language is generally thought to involve interactive subcomponents that support comprehension via multiple input modalities (e.g., spoken words, pictures, gestures, written words, tactile input, environmental sounds), and that support expression through various output modes (e.g., speaking, drawing, gesturing, writing). Detailed discussion of models of language processing is beyond the scope of this chapter; however, the practical suggestions below include methods for assessment of single-word knowledge as well as comprehension and production of sentences.
5.1.3 Assessment of Single-Word Comprehension
When comprehension is impaired, the SLP must diagnose both the type and the severity of the disturbance. Individuals with less severe forms of comprehension impairment may be perceived as uncooperative when they do not respond appropriately to requests or instructions that contain words or syntactic constructions they do not comprehend. An important role for the SLP is educating family members and health care staff about the PWA’s level of impairment and strategies to maximize comprehension. Individuals with Broca’s, conduction, transcortical motor, and anomic aphasia subtypes, although categorized as having generally spared comprehension, nevertheless may have mild comprehension impairment that interferes with functional communication. Also, sentence comprehension may be severely impaired even if single-word comprehension is spared.
▶ Fig. 5.1 represents cognitive processes thought to be involved in comprehension of single words through various input modalities. 10 Within the framework in ▶ Fig. 5.1, normal comprehension occurs following perception of a stimulus, recognition of the stimulus as familiar (at the level of the input lexicon or object recognition units), and activation of its meaning within semantic memory. 11 Note that recognition can occur without comprehension (i.e., the PWA may recognize a stimulus as familiar but not understand its meaning).
Fig. 5.1 Schematic of cognitive processes involved in single-word comprehension Adapted from Caramazza A, Hillis AE, Rapp BC, Romani C. The multiple semantics hypothesis: multiple confusions? Cogn Neuropsychol 1990;7:161–189. 12
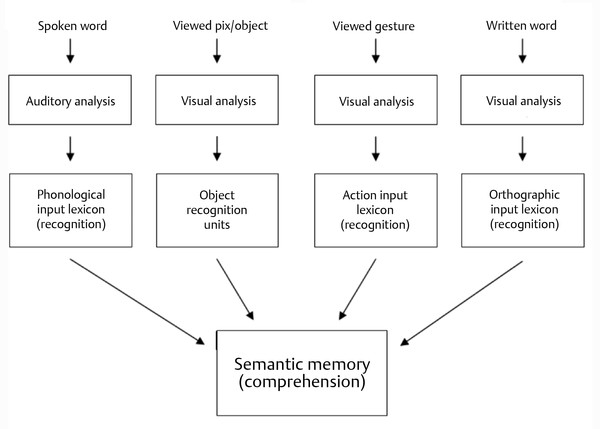
When semantic memory is disrupted, comprehension from all input modalities is impaired. Alternatively, comprehension can be disrupted from only one input modality in the context of normal comprehension via other modalities. 13 For example, specific impairment to visual object processing could impair visual perception, visual recognition, and/or association of the viewed object or picture with semantics. Administration of the Birmingham Object Recognition Battery 14 (BORB) would allow the SLP to assess visual object processing in detail.
In general, the ability to recognize as familiar a stimulus from any input modality can be measured using a task of “lexical decision” (i.e., real or not real). For example, in an auditory or written lexical decision task, the clinician presents a real word or a nonword (e.g., flig) and the PWA decides if the stimulus is real or not real. 15 Real words that are more common (i.e., high frequency) are easier to accept as real than real words that are less common (i.e., low frequency). Therefore, patients with impaired recognition may demonstrate a pattern of better performance given high-frequency words as compared to low-frequency words. With impaired recognition of visual stimuli, errors are often visually related to the target; impaired recognition of spoken stimuli often yields phonologically related errors.
Poor comprehension due to impaired semantic memory is generally thought to result from poor activation of the semantic features that differentiate one single-word concept from another. 16 Individuals with semantic memory impairment may be able to comprehend the general semantic category of a word (e.g., animal) although they are unable to comprehend more specific details of meaning that distinguish the target word (e.g., zebra) from a semantically related word (e.g., giraffe). With impaired semantic memory or impaired access to semantic memory, errors often are semantically related to the target. 10
Comprehension is one of the psycholinguistic features of aphasia that can be measured in detail using the PALPA, 7 noted above. For example, the PALPA includes stimuli for measuring synonym judgments (i.e., deciding if two words have the same meaning). Also, the SLP can assess severity of comprehension impairment by systematically manipulating the array size and types of foils included in word comprehension tasks. In general, the difficulty of a semantic comprehension task increases with the semantic relatedness of choices presented and with increasing number of choices.
▶ Table 5.2 contains selected comprehension tasks in order of increasing task difficulty. 17 For example, among the matching tasks listed, a difficult version suitable for detecting higher-level comprehension impairments is the semantic associate matching task in which the word stimulus does not have a direct picture match but must be matched to a picture associated in meaning with the word stimulus (e.g., matching “horse” to picture of saddle). The BORB, noted above, and the Pyramids and Palm Trees Test 18 include measures of semantic associate matching.
Category sorting (listed in increasing task difficulty) |
Sort stimuli into distant semantic categories (e.g., transportation versus food) |
Sort stimuli into close semantic categories (e.g., fruits versus vegetables) |
Sort stimuli within semantic category (e.g., winter versus summer clothing) |
Matching tasks (listed in increasing task difficulty) |
Direct match of word to its picture (e.g., match “horse” to picture of horse) |
Given 2 choices: target and 1 unrelated foil |
Given 3 or more choices: target and 2 or more unrelated foils |
Given 2 choices: target and 1 semantically related foil |
Given 3 or more choices: target and 2 or more semantically related foils |
Match word to its semantic associate (e.g., match “horse” to picture of saddle) |
5.1.4 Assessment of Sentence Comprehension
For many PWAs, impaired understanding of sentences presents a functional obstacle to conversational interactions and even the ability to follow simple instructions. The ability of a PWA to understand spoken sentences can be disrupted by different cognitive or syntactic impairments. Often, active canonical subject-verb-object (SVO) sentences (e.g., “The girl is pushing the boy”) are easier for a PWA to comprehend than are noncanonical sentence structures, such as passive sentences (e.g., “The boy is pushed by the girl”) or object cleft constructions (e.g., “It was the boy that the girl pushed”). 19
One method for differentiating the type of sentence comprehension deficit in aphasia is to administer the sentence-picture matching task. For example, for the target picture depicting “The dog is chasing the girl,” the distracter pictures can include the incorrect noun (i.e., The dog is chasing the car) or verb (i.e., The dog is licking the girl) to allow detection of poor comprehension of single words in the sentence. For this same target sentence, including the distracter picture for “The girl is chasing the dog” would allow detection of difficulty in comprehending who is doing what to whom (i.e., thematic role assignment). If stimuli do not include semantically reversible sentences in which either noun (e.g., girl or dog) could be doing the action (e.g., chasing), then the clinician may miss a deficit in thematic role assignment. 20
A variety of sentence comprehension measures for aphasia are available. For example, other current approaches to assessing sentence comprehension are described by Myers and Blumstein. 21
5.1.5 The Influence of Other Cognitive Deficits on Comprehension
Attention, working memory, and executive functions are necessary for normal comprehension of single words and sentences, particularly in functional communication involving multiple conversational partners and distracting environments. Among aphasia researchers, there are differing perspectives on the contribution of reduced working memory or processing capacity 22 versus impaired language representation 23 on sentence processing, and how cognitive deficits in these areas can be assessed and treated in a PWA. 24, 25 Cognitive assessment results reported by the neuropsychologist typically are available to the SLP in medical records. Also, the SLP can observe the PWA in a variety of communication contexts, gaining real-world information about how overall cognitive status may be affecting functional use of communication.
Impaired verbal working memory in a PWA can be detected using tasks like digit span (i.e., repeating number sequences after the examiner). 26 For a PWA with impaired repetition, the digit-span task can be modified into a pointing-span task in which the examiner says the numbers aloud and the PWA points to the corresponding numbers instead of repeating them aloud. 27 Also, the sentence-to-picture matching task (described above) can be altered to allow detection of the influence of impaired verbal working memory on sentence comprehension. 28 For example, the same sentence construction can be presented aloud both with and without the “padding” of additional words; modifiers would not provide information to aid sentence matching but would increase sentence length and thus the demand on working memory. For example, the PWA can be asked to match the sentence “The dog is chasing the girl” to the target picture from an array of pictures, and later asked to match a “padded” version of the same sentence (e.g., “The large dog is playfully chasing the tall girl”) to a choice of pictures. 28 For some PWAs with good single-word comprehension but poor sentence comprehension, the reason why the sentence is misunderstood may be its length (i.e., working memory demand) rather than the complexity of the syntax.
5.1.6 Right Hemisphere Damage and Comprehension
Patients with right hemisphere lesions may not exhibit the lexical-semantic or sentence-processing deficits described above, but nevertheless may have difficulty with many forms of comprehension. Right hemisphere damage can disrupt comprehension of the central themes of discourse, connotative word meanings, figurative language, inferences, humor, and emotional and linguistic prosody. 29, 30 An evidence-based systematic review of communication treatments for right hemisphere brain damage is provided by Blake et al. 31
5.1.7 Assessment of Verbal and Written Naming
Spontaneous verbal or written expression requires activation of semantic memory and then abstract whole-word (i.e., lexical) forms for spoken or written language 10 (see ▶ Fig. 5.2). These semantic and lexical elements are also used for verbal or written naming in response to incoming stimuli, such as auditory definitions, gestures, pictures, or written words. In addition to this activation of whole-word lexical forms, oral reading or spelling can be accomplished via sublexical conversion from grapheme to phoneme (reading) or from phoneme to grapheme (spelling). Irregularly spelled words (e.g., yacht) can be processed correctly only via lexical activation, nonwords (e.g., flig) or unfamiliar words can be pronounced via sublexical translation, and regularly spelled words (e.g., hotel) can be processed correctly either way. Semantic concepts can also be expressed through additional modes, such as gesture, drawing, and facial expressions, which may become critical modes of communication for aphasia patients who have expressive impairments in the verbal and written modes ( ▶ Fig. 5.2). Lexical or sublexical information for the various forms of expression presumably is held in working memory during subsequent motor programming for expression. 32
Fig. 5.2 Schematic of cognitive processes involved in single-word expression. Adapted from Caramazza A, Hillis AE. Where do semantic errors come from? Cortex 1990;26(1):95–122. 33
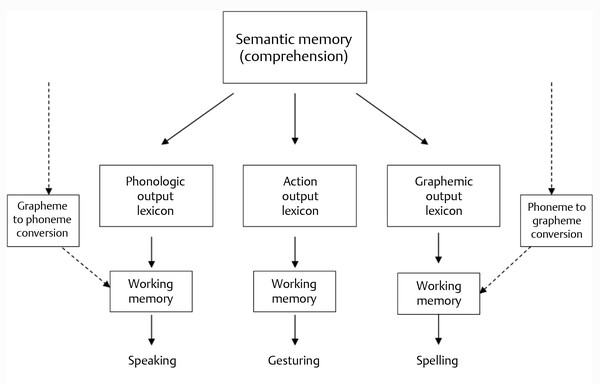
Impaired semantic memory will result in impaired output across expressive modes, and frequent semantic errors (e.g., “chair” for “table”). If semantic memory is intact, semantic errors still can result from poor egress from semantics to the output lexicon or from an impaired output lexicon. 33 Disruption to the output lexicon for phonology also will result in phonological errors in speech 34 and poor performance in discriminating rhymes 35 (i.e., yes/no judgments about whether two written words rhyme). When the graphemic output lexicon is impaired, spelling errors will be related to the target semantically (e.g., c-o-w for “horse”) or orthographically (i.e., 50% or more of the target letters, such as w-e-a-t-h-e-r for “wheat”). Impaired working memory can affect phonological or graphemic knowledge, resulting in errors in which the initial position is correct, with worse performance in the middle and final positions of the target word. 36
5.1.8 Assessment of Sentence Production
Many persons with aphasia experience difficulty formulating sentences, producing little or no grammatical structure. If they manage to produce a verb, sentence structure is often simplified into SVO canonical order, with particular difficulty producing noncanonical sentences, such as the passive form. 37 Grammatical morphology (e.g., verb inflections) is often impaired. 38 Measures of sentence processing, such as The Northwestern Assessment of Verbs and Sentences, 39 allow subtypes of sentence production impairment to be differentiated.
One way to evaluate the differential effects of impaired word retrieval versus impaired sentence formulation in aphasia is to ask the PWA to produce a sentence beginning with a given phrase. That is, to elicit an active sentence corresponding to a presented action picture (e.g., “The dog is chasing the girl”), the clinician asks the PWA to “Start with the dog” (the agent of the action). In a later trial, the clinician attempts to elicit a passive sentence for this action picture by asking the PWA to produce a sentence and to “Start with the girl” (the object of the action). 40 The PWA who is able to produce a correct active sentence, such as “The dog is chasing the girl,” has demonstrated good word-retrieval skills; the inability to produce those words in a passive construction (e.g., “The girl is chased by the dog”) can then be attributed to difficulty in formulating the passive form rather than simply anomia. 41
Discourse in a PWA can be assessed using a story-retelling task and Quantitative Production Analysis 42 (QPA). To elicit retelling of the Cinderella story, the clinician would silently review the pictures from the story with the client to help the client recall the order of the story, and then close the pictures and ask the PWA to retell the story. Aside from QPA, there are a variety of methods for analyzing language samples in a PWA. 43 Sample analyses of a large, shared database of transcripts of PWAs retelling the Cinderella story are available online 44 (AphasiaBank).
5.1.9 Assessment of Functional and Social Communication
Observing the PWA in natural communication situations may provide valuable information about effective communication strategies for that individual. As stated above, one goal of comprehensive aphasia assessment is to identify areas of communication strength, which the PWA may learn to draw upon to reach his or her life participation goals. Two available measures of functional communication are the Communication Abilities in Daily Living 45 (CADL-2) and the Communicative Effectiveness Index 46 (CETI). Importantly, the SLP works collaboratively with the PWA to assess baseline life participation and to set communication goals. 47
5.1.10 Multicultural Issues in Aphasia Assessment
Persons with aphasia have diverse language backgrounds and diverse cultures that influence the process of aphasia assessment. Some formal test measures are available in a variety of languages, 48 but the SLP may require assistance from an interpreter for test administration and interpretation. Similarly, a cultural advisor or family member of the PWA may be able to assist the SLP in understanding cultural perspectives that influence the PWA’s reaction to assessment and response to treatment. “Dynamic assessment” of aphasia, which focuses on identifying factors that enhance the individual’s communication, may help the SLP to differentiate language differences from language disorders. 49 For example, the PWA may demonstrate the ability to learn a communication strategy given initial modeling and cuing, before progressing to independent use of the strategy.
5.2 Perspectives on Aphasia Rehabilitation
The goal of aphasia rehabilitation is to assist persons with aphasia, within the context of their environment and the type and extent of CNS damage, to reach their full potential in communication. Toward this end, the SLP tailors treatment approaches to the unique communication needs and concerns of each individual. Aphasia intervention addresses impairments in cognitive-linguistic function, language skill, and real-life adaptation to reduced language skill, but the communication strengths of the PWA also are emphasized. The overall objective of aphasia treatment is that therapy gains will be generalized to functional communication contexts. 50
As summarized by Rothi, 51 two processes determine progress in aphasia rehabilitation after brain injury: reactive plasticity of neural tissues and restoration of lost knowledge through “experience-based, behavioral interventions.” Aside from specific subtypes of aphasia rehabilitation (described below), two general areas of focus in current aphasia research are (1) examining the effects of varying treatment intensities, 52 and (2) evaluating the relative positive or negative effects of compensatory communication behaviors on rehabilitation of a desired target behavior. 53, 54 Also, there is current interest in how training of related cognitive abilities, such as working memory 55 or attention, 56 may influence rehabilitation in PWAs who have multiple cognitive deficits.
5.2.1 The Continuum of Care
The approach to aphasia rehabilitation necessarily varies with the stroke survivor’s stage of recovery and the setting in which intervention occurs. The SLP may be involved in providing care for individuals with aphasia at one or more of the following stages of recovery: acute care (acute hospital); subacute care (extended care facility); inpatient rehabilitation (rehabilitation hospital or unit); home care (patient’s home); and outpatient rehabilitation (rehabilitation center). In post-acute settings, rehabilitation services often are implemented by multidisciplinary teams in which the SLP interacts closely with professionals in rehabilitation medicine, neurology, occupational therapy, physical therapy, nursing, neuropsychology, and social work in coordinating patient care.
Evolution of aphasia (described above) requires the SLP to be flexible in modifying treatment goals and in systematically altering the difficulty level of treatment tasks to meet the current needs of the individual. As the aphasia evolves, new therapy issues and concerns arise. For example, although improving auditory comprehension is a positive sign of evolution from Wernicke’s aphasia to conduction aphasia, individuals at this stage of recovery are likely to experience increased frustration as they begin to notice their own speech errors and attempt self-correction. It is important to note that the underlying aphasia subtype may remain the same even when the individual’s functional communication improves significantly as a result of treatment. For example, an individual with anomic aphasia may remain anomic, but may learn effective strategies to compensate for the anomia.
5.2.2 Evidence-Based Practice
In determining the approach to aphasia intervention for each individual, the SLP considers the best available evidence from the scientific literature, clinical practice guidelines, and expert opinion, and the unique needs, environment, and perspectives of the PWA and his or her family. 57 One resource for evidence-based practice guidelines and systematic reviews is the ASHA Website at www.asha.org. Suggestions for applying the principles of evidence-based aphasia therapy in the outpatient clinical setting are offered by Fucetola et al. 58
5.3 Rehabilitation of Impaired Comprehension
Rehabilitation of comprehension can be designed to target the cognitive-linguistic component(s) affected (e.g., semantic memory), the general skill area affected (e.g., auditory comprehension), or adaptation to the real-life effects of reduced comprehension. Impaired comprehension is not limited to the global, Wernicke’s, transcortical mixed, and transcortical sensory aphasia subtypes; as noted above, comprehension may be compromised in the remaining subtypes, especially sentence comprehension. The SLP and other communication partners of the PWA will need to incorporate multiple input modalities in attempts to convey meaning to the person with severely impaired comprehension. Verbal utterances that contain high-frequency, concrete words presented alone or in short, simple, grammatical constructions are more likely to be understood than more complex verbalizations. Slowing the rate of speech can increase auditory comprehension for the PWA. 59
5.3.1 Treating Comprehension of Pictures and Objects
Pointing to pictures or objects in the environment may be sufficient to convey some ideas to the PWA with severely reduced comprehension. However, there is a safety risk among these individuals in that they may not understand the functions associated with some objects or tools in the environment (i.e., conceptual apraxia). The SLP can identify any potential safety risk 60 and counsel family members to avoid the PWA’s incorrectly selecting an item to complete a task (e.g., selecting a sharp item to brush teeth).
An individual with a semantic memory deficit may benefit from a variety of treatment tasks that require activation of semantic features. 61, 62, 63, 64 Simple matching tasks involving pictures provide a means of activating semantic memory in a PWA with poor comprehension. As described below regarding gesture or word stimuli, the difficulty of the picture-matching task can be modified by changing the array size or the types of distracters used. For example, including only one distracter that is unrelated to the target is appropriate for a PWA with severely impaired semantic memory, whereas picture-matching tasks that include multiple semantically related distracters may be suitably challenging for a PWA with mild semantic impairment.
The simple task of sorting pictures into two distantly related semantic categories (e.g., animals versus tools) can be modeled by the SLP and the instructions conveyed nonverbally to the PWA. This sorting task provides practice in activating semantic memory, and the difficulty level can be systematically increased as performance improves by using semantic categories that require more semantic specification to differentiate (e.g., kitchen tools versus yard tools). Because semantic memory is central to comprehension across input modalities ( ▶ Fig. 5.1) improved semantic activation in picture-sorting or matching tasks would be predicted to result in improved semantic activation from other input modalities, such as words and gestures.
An individual with a very severe comprehension deficit may be unable to perform even the least difficult sorting or matching tasks, despite extensive modeling. In this case, the clinician can probe the PWA’s ability to perform the more basic task of matching two physically identical objects presented with one unrelated distracter (e.g., two identical cups and a pencil). If the PWA is unable to match at this more basic level when assessed across several sessions, they may not be ready to participate in language treatment. However, with aphasia evolution, this task is a possible starting point for comprehension treatment during the following weeks or months.
5.3.2 Treating Gesture Comprehension
Not all PWAs understand the symbolic nature of gestures, or the meaning of gestures. Visual Action Therapy 65 (VAT), a structured nonverbal therapy program designed to assist the PWA to comprehend gestures, begins with simple tracing tasks and progresses systematically toward gesture comprehension and production. The initial stages of VAT can be an excellent starting point for intervention with the PWA with severely reduced comprehension. Another approach to facilitating gesture comprehension is through gesture-matching tasks; for example, an easier version in which the number of choices is very limited and the distracters are unrelated to the target (e.g., the clinician could present gesture for “drink” and choice of cup or pencil).
5.3.3 Treating Comprehension of Single Words
There is evidence that word-matching tasks can lead to improved auditory comprehension in aphasia, for example, in the individual with Wernicke’s aphasia and severe semantic impairment reported by Grayson et al. 63 A simple version of spoken word-to-picture matching is presenting the client with a spoken word (e.g., “apple”) and pictures of the target and one unrelated distracter (e.g., car). This task also can be presented as written word-to-picture or spoken-word-to-written-word matching. Systematic manipulation of task difficulty allows the clinician to extend the task as the performance of the PWA improves. First, the array size can be increased to three or more (e.g., the spoken word “apple” can be presented with a choice of apple, car, and blanket) while keeping all distracters unrelated to the target. Second, the semantic relatedness of the distracters to the target can be increased (e.g., the spoken word “apple” can be presented with a choice of apple or grapes). As performance improves, the task can incorporate semantically related distracters in a large array size (e.g., present spoken word “apple” with choice of apple, grapes, banana, and pear). In this way, the matching task can be adapted to place increasing demands on the PWA’s ability to make semantic distinctions.
Improved auditory comprehension in a person with global aphasia and severely impaired semantic processing was reported after treatment focused on teaching superordinate features of semantic categories (e.g., animals) followed by a treatment phase focused on specific semantic features of items within a category. 61 Auditory comprehension improved in two PWAs with semantic impairment following computerized training in word-picture matching involving semantic distracters. 66 Improved auditory comprehension performance on a short form of the Token Test 67 resulted in four individuals with Wernicke’s aphasia following eleven treatment sessions including verbal matching tasks. 68
One approach to facilitating semantic processing is semantic feature analysis 69 (SFA), in which the PWA generates semantic features of a given concept. This has been used as a treatment for impaired naming, but its focus on semantic memory has the potential to improve comprehension as well. Also, SFA or variations of SFA have had positive results even when the PWA analyzes semantic features generated by others rather than the PWA’s generating these features. 70
Significant improvement in auditory comprehension was observed in a group of 28 individuals with chronic aphasia following constraint-induced therapy involving verbal production tasks and a restraint on alternative, nonverbal communication. 71 The treatment resulted in significant improvement in auditory comprehension as measured by average scores on the Token Test. 67
There is recent evidence that impaired comprehension in aphasia can improve in some PWAs after intervention aimed at improving attention and/or working memory. 72, 73 Ongoing studies of attempts to manage impaired attention associated with traumatic brain injury may have applications to aphasia. 74
5.3.4 Treating Modality-Specific Comprehension Deficits
Semantic tasks using one form of input have the potential to improve semantic processing from multiple input modalities, because semantic memory is central to comprehension from all input modalities ( ▶ Fig. 5.2
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


