Chapter 13 Antibacterial drugs
Classification
Inhibition of cell wall synthesis
β-lactams
the structure of which contains a β-lactam ring. The major subdivisions are:
• Penicillins, whose official names usually include, or end in, ‘cillin’.
• Cephalosporins and cephamycins, which are recognised by the inclusion of ‘cef ’ or ‘ceph’ in their official names. In the UK recently all these names have been standardised to begin with ‘cef’.
Other subcategories of β-lactams include:
Other inhibitors of cell wall synthesis include vancomycin and teicoplanin.
Inhibition of cell wall synthesis
β-lactams
Penicillins
Mode of action
Penicillins act by inhibiting the enzymes (penicillin binding proteins, PBPs) involved in the cross-linking of the peptidoglycan layer of the cell wall, which is weakened, and this leads to osmotic rupture. Penicillins are thus bactericidal and are ineffective against resting organisms which are not making new cell wall. The main defence of bacteria against penicillins is to produce enzymes, β-lactamases, which hydrolyse the β-lactam ring. Other mechanisms that have been described include modifications to PBPs to render them unable to bind β-lactams, reduced permeability of the outer cell membrane of Gram-negative bacteria, and pumps in the outer membrane which remove β-lactam molecules. Some particularly resistant bacteria may possess several mechanisms that act in concert. The remarkable safety and high therapeutic index of the penicillins is due to the fact that human cells, while bounded by a cell membrane, lack a cell wall. They exhibit time-dependent bacterial killing (see p.164).
Narrow-spectrum penicillins
Benzylpenicillin
Benzylpenicillin (t½ 0.5 h) (penicillin G) has to be given with spaced doses that have to be large to maintain a therapeutic concentration, but the large therapeutic ratio of penicillin allows the resulting fluctuations to be tolerable.1 Benzylpenicillin is eliminated by the kidney, with about 80% being actively secreted by the renal tubule and this can be blocked by probenecid.
Antistaphylococcal penicillins
Examples of agents stable to staphylococcal β-lactamases include:
• Flucloxacillin (t½ 1 h) is better absorbed and so gives higher blood concentrations than does cloxacillin. It may cause cholestatic jaundice, particularly when used for more than 2 weeks or given to patients > 55 years.
• Cloxacillin (t½ 0.5 h) has been withdrawn from the market in some countries, including the UK.
• Methicillin and oxacillin: their use is now confined to laboratory sensitivity tests. Identification of methicillin-resistant Staphylococcus aureus (MRSA) in patients indicates the organisms are resistant to all β-lactam antibiotics and often to other antibacterial drugs.
Cephalosporins
Mode of action
is that of the β-lactams, i.e. cephalosporins impair bacterial cell wall synthesis and hence are bactericidal. They exhibit time-dependent bacterial killing (see p. 164).
Pharmacokinetics
Usually, cephalosporins are excreted unchanged in the urine, but some, including cefotaxime, form a desacetyl metabolite which possesses some antibacterial activity. Many are actively secreted by the renal tubule, a process which can be blocked with probenecid. As a rule, the dose of cephalosporins should be reduced in patients with poor renal function. Cephalosporins in general have a t½ of 1–4 h although there are exceptions (e.g. ceftriaxone, t½ 8 h). Wide distribution in the body allows treatment of infection at most sites, including bone, soft tissue, muscle and (in some cases) CSF. Data on individual cephalosporins appear in Table 13.1.
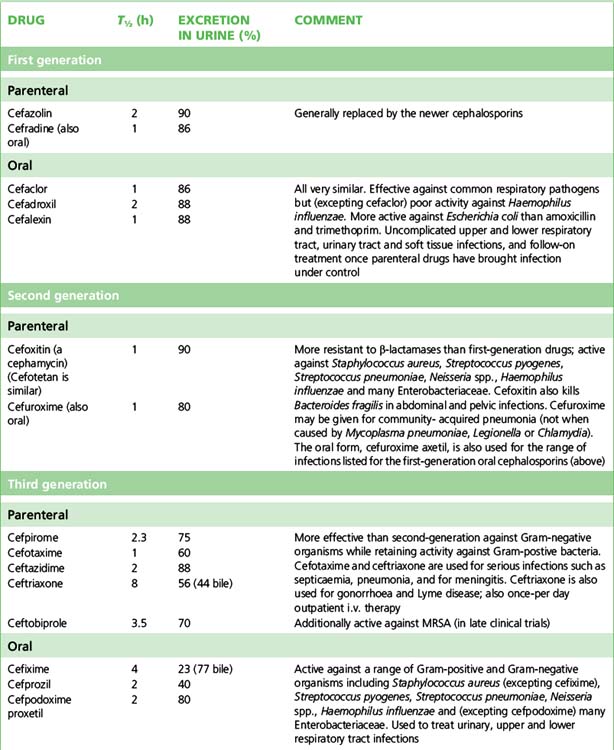
Classification and uses
The cephalosporins are conventionally categorised by ‘generations’ sharing broadly similar antibacterial and pharmacokinetic properties; newer agents have rendered this classification less precise but it retains sufficient usefulness to be presented in Table 13.1.
Adverse effects
Cephalosporins are well tolerated. The most usual unwanted effects are allergic reactions of the penicillin type, and gastrointestinal upset. Overall the rate of cephalosporin skin reactions such as urticarial rashes and pruritis lies between 1% and 3%. There is cross-allergy between penicillins and cephalosporins involving up to 10% of patients; if a patient has had a severe or immediate allergic reaction or if serum or skin testing for penicillin allergy is positive (see p. 176), then a cephalosporin should not be used. Pain may be experienced at the sites of i.v. or i.m. injection. If cephalosporins are continued for more than 2 weeks, reversible thrombocytopenia, haemolytic anaemia, neutropenia, interstitial nephritis or abnormal liver function tests may occur. The broad spectrum of activity of the third generation cephalosporins may predispose to opportunist infection with resistant bacteria or Candida albicans and to Clostridium difficile diarrhoea. In the UK, reduction of broad-spectrum cephalosporin use is one component of the bundle of measures aimed to reduce the incidence of Clostridium difficile-associated diarrhoea. Ceftriaxone achieves high concentrations in bile and, as the calcium salt, may precipitate to cause symptoms resembling cholelithiasis (biliary pseudolithiasis).
Other inhibitors of cell wall synthesis and membrane function
Vancomycin
Daptomycin
(t½ 9 h) is a recently released lipopeptide antibiotic, naturally produced by the bacterium Streptomyces roseosporus which was first isolated from a soil sample from Mount Ararat in Turkey.3 It has activity against virtually all Gram-positive bacteria, including penicillin-resistant Streptococcus pneumoniae and MRSA, regardless of vancomycin resistance phenotype. It is unable to cross the Gram-negative outer membrane, rendering these bacteria resistant.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


