Anatomy and physiology, or A&P, are subjects that just about every student assumes will be among the most difficult to study. True, it requires a lot of memorization, and many people don’t have the patience to study, tending to look for shortcuts and cheat sheets and so forth to pass their tests instead. Those of you considering the easy way out need to ask yourself this question: Why is knowledge of anatomy and physiology important for the surgical technologist?
Here’s why: The surgical technologist, a member of an advanced allied health profession, must have a basic working knowledge of A&P to do the job safely and well. Knowing the parts and systems of the human body and how they work will help you understand and anticipate the steps of surgical procedures much more effectively.
We believe that studying A&P productively requires patience and consistency. There’s no denying that this subject matter is complicated, but there are ways in which you can learn and retain the material— you just have to be consistent. This will help you become familiar with the subject, and familiarity fosters memorization and understanding.
One means of improving your understanding and recall is to draw pictures of what you’re studying—or, if you’re not an artist, just cut out pictures of the anatomy and stick them around your study room. Look at them every day. Trust me: our brains function just like a camera, and the more time you spend looking at the images, the more deeply they will be registered in your memory bank.
Complicated though it might be, anatomy and physiology is also fun. Here’s just a tiny sampling of fascinating A&P facts:
• Let say you decide to try eating while standing on your head. Even upside down, the smooth muscle of the esophagus will continue to do its job, moving in a wavelike motion, until the food is deposited safely in your stomach. (It takes 2 to 5 seconds for food to travel from the mouth to the stomach.)
• Over a 24-hour period, the salivary glands will produce 1.7 L of fluid.
• In the average adult, 11.5 L of food, liquids, and digestive juices makes its way through the digestive system over the course of 24 hours, but only 100 mL is lost in feces.
• Your entire digestive system, from mouth to anus, is 30 feet long; the small intestine is about 22 feet (7 m) long.
• The hydrochloric acid found in our stomachs is the same substance used by masons to clean bricks.
• The human gastrointestinal system plays host to more than 500 species of bacteria.
• Intestinal gas, or flatus, is a combination of swallowed air and the gases produced by the fermentation of bacteria in the gastrointestinal tract. Certain components of food can’t be broken down or absorbed by the digestive system, and those substances are simply pushed along the tract and into the large intestine (a.k.a. the colon). Hordes of intestinal bacteria in the colon go to work, releasing a variety of gases in the process, including carbon dioxide, hydrogen, methane, and hydrogen sulfide, which gives flatulence its rotten-egg stench.
Preparing for a Certification Exam

(Copyright © Wavebreakmedia Ltd/Wavebreak Media/Getty Images.)
Before we get started on our review, let’s talk about what’s going to be asked of you, in terms of anatomy and physiology, on your certification examination. Here are the expectations set forth in the outline provided by the NBSTSA.
• Use appropriate medical terminology and abbreviations.
• Demonstrate knowledge of these anatomical systems and their physiology as they relate to the surgical procedure:
• Cardiovascular
• Gastrointestinal
• Endocrine
• Integumentary
• Lymphatic
• Muscular
• Neurological
• Peripheral vascular
• Reproductive
• Pulmonary
• Otorhinolaryngologic
• Skeletal
• Genitourinary
• Ophthalmic
• Identify the following surgical pathologies:
• Abnormal anatomy
• Disease process
• Traumatic injuries
• Malignancies
In this chapter we’ll be making our way through these lists to ensure that you can tie anatomy and physiology together in the context of pathologic conditions treated with surgery. Let’s get to work!
Cardiovascular System
CABG (Coronary Artery Bypass Graft)
See Fig. 2.1. What parts of the anatomy are affected by this procedure?
• Aorta (becomes occluded, necessitating CABG)
• Sternum (sternotomy performed to provide access)
• Coronary artery (subjected to coronary arteriotomy)
• Internal mammary artery (harvested as a graft)
• Saphenous vein (harvested as a graft)
Remember, the NBSTA exam will require you to know the surgical pathologies, which include abnormal anatomy, disease process, traumatic injuries, and malignancies, if any, related to the procedure or to find a better way to understand why the patient is scheduled for CABG.
Mapping
Remember the mapping method we discussed in the Introduction? Here’s where we start using it. Let’s map some commonly performed cardiovascular procedures.
Aortic Valve Replacement
What parts of the anatomy are affected by this procedure?
• Ascending aorta (becomes occluded)
• Aortic valve (requires replacement)
• Sternum (sternotomy performed to provide access)
Mapping

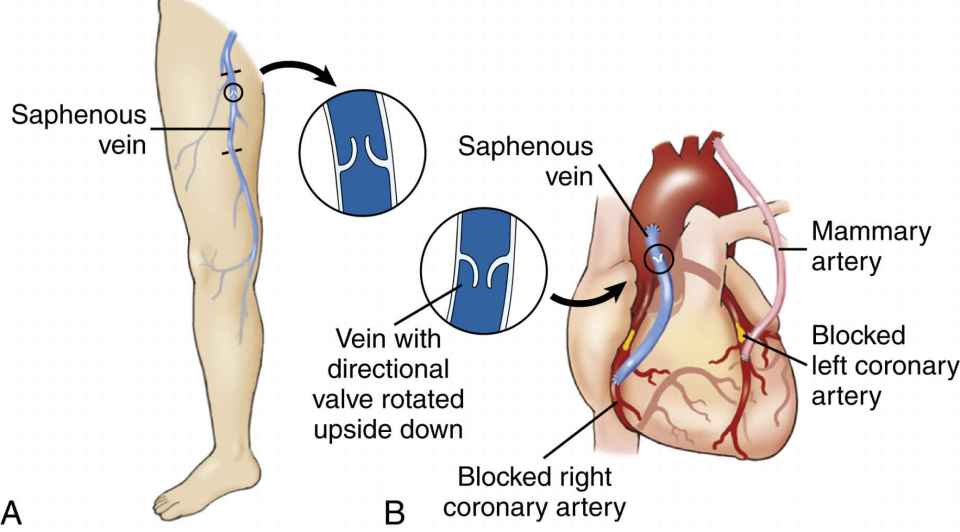
FIG. 2.1 Coronary artery bypass graft (CABG) surgery. (From Shiland BJ: Medical Terminology & Anatomy for ICD-10 Coding, ed 2, 2015, St Louis, Mosby.)

FIG. 2.2 Mitral valve prolapse. The normal mitral valve (upper left) prevents backflow of blood from the left ventricle into the left atrium during ventricular systole (contraction). The prolapsed mitral valve (right) permits leakage because the valve flaps billow backward, parting slightly. The photo inset shows the ballooning (arrow) of the mitral valve into the atrium. (Drawings from Patton KT, Thibodeau GA: The Human Body in Health and Disease, ed 6, 2014, St Louis, Mosby; photo courtesy of William D Edwards, MD, Mayo Clinic, Rochester, MN.)
Mitral Valve Replacement
See Fig. 2.2. What anatomy is affected by this procedure?
• Ascending aorta (becomes occluded)
• Mitral valve (a.k.a. bicuspid valve, between the left atrium and left ventricle)
• Sternum (sternotomy for the purpose of access)
Mapping
Let’s map this aortic procedure:
Resection of Aneurysm of the Ascending Aorta
See Fig. 2.3. What parts of the anatomy are affected by this procedure?
• Aorta
• Sternum (sternotomy performed to provide access)
• Aortic valve
• Femoral artery (used as a graft)
• Coronary arteries

Mapping
Here you can see how this procedure maps:


Heart Transplantation
See Fig. 2.4. What parts of the anatomy are affected by this procedure?
• Sternum (sternotomy performed to provide access)
• Pulmonary veins
• Pulmonary arteries
• Orthotopic heart
Mapping
Let’s lay the procedure out in a map:
Other Cardiovascular Procedures
Now it’s your turn to do some mapping! Using the template provided on the Evolve Resources site, map out each procedure—name, related anatomy, abnormal anatomy, and pathology—for each of the following cardiac procedures.
• Cardiac pacemaker insertion
• Endovascular repair of thoracic aneurysm
• Pericardial window
• Insertion of a ventricular assist device (VAD)
Gastrointestinal System
The gastrointestinal system comprises much more than just the stomach and intestines (Fig. 2.5). Let’s have a quick review of the areas and organs of the gastrointestinal tract before we start mapping the surgeries that affect them.
Divisions of the Abdomen
Quadrants
See Fig. 2.6.
• Right upper quadrant
• Right lower quadrant
• Left upper quadrant
• Left lower quadrant
Regions
See Fig. 2.7.
• Right hypochondrium
• Right lumbar region
• Right iliac fossa region
• Epigastrium
• Umbilical region
• Hypogastric or suprapubic region
• Left hypochondrium
• Left lumbar region
• Left iliac fossa region
Tissue Layers: Superficial to Deep
• Skin
• Subcutaneous fatty tissues
• Fascia
• Muscle
• Peritoneum
Organs of the Gastrointestinal System
Digestive Tract
These organs extract nutrients and water from food for the nourishment of the body and then get rid of any waste material remaining.
• Esophagus: smooth muscle–lined tube through which chewed food, liquids, and saliva travel from the mouth to the stomach by means of peristalsis

FIG. 2.5 Location of the digestive organs. (From Patton KT, Thibodeau GA: The Human Body in Health and Disease, ed 6, 2014, St Louis, Mosby.)

• Small intestine: long tubular organ that receives partially digested food (chyme) from the stomach, as well as bile from the liver and digestive enzymes from the pancreas to further break down the food into nutrients
• Large intestine (a.k.a colon): a second long tubular organ; receives mostly digested food from the small intestine, extracts water from the digested food, and forms waste material into feces

• Rectum: final section of the large intestine, where feces are stored before expulsion
• Anus: muscular ring through which feces are expelled from the body; terminus of the digestive tract.
Accessory Digestive Organs
Liver
See Fig. 2.8. The liver has many responsibilities:
• Processing blood to remove nutrients, toxins, and medications
• Storing energy in the form of glycogen
• Storing vitamins and minerals and releasing them as the body needs them
• Producing proteins needed for blood clotting
• Producing bile, which aids digestion
Gallbladder
This structure stores the bile that the liver produces until it is needed for digestion.
Pancreas
This organ belongs to both the digestive and endocrine systems (Fig. 2.9).
• The pancreas contains structures known as the islets of Langerhans, made up of cells that secrete hormones:
• Alpha cells secrete glucagon.
• Beta cells secrete insulin.
• The pancreas also produces an enzyme that aids in digestion, as well as bicarbonate, which neutralizes stomach acid before it reaches the small intestine.
Spleen
See Fig. 2.10. Like the liver and pancreas, this organ does several jobs:
• It holds a reserve of blood to counteract hemorrhagic shock.
• It removes from circulation and destroys aged red blood cells.
• It makes antibodies to aid immune response.
• It stores half the body’s monocytes, which differentiate into several cell types as needed.
Gastrointestinal Surgeries
Hernia Repair
A hernia is a protrusion of abdominal contents through a weakened area of the abdominal wall (Fig. 2.11).

FIG. 2.8 The liver. A, anterior view. B, turned up to show posterior surface. (From Waugh A, Grant A: Ross and Wilson Anatomy & Physiology in Health and Illness, ed 12, Edinburgh, 2014, Churchill Livingstone.)

What parts of the anatomy are affected by this procedure? That depends on the type of hernia.
• Omentum (most commonly)
• Small intestine
Mapping
Let’s organize the pertinent information on hernia repair into a map:

FIG. 2.10 The spleen, composed of white pulp and red pulp. (From Herlihy B: The human body in health and illness, ed 5, St Louis, 2014, Saunders.)

Esophageal Procedures
See Fig. 2.12. What parts of the anatomy are affected by these procedures?
• Esophagus
• Fundus of the stomach
Mapping
Here’s the mapping for three procedures involving the esophagus:

FIG. 2.11 Common types of abdominal hernias. A, Umbilical hernias result from a weakness in the abdominal wall around the umbilicus. An incisional hernia is herniation through inadequately healed surgery. In a femoral hernia, a loop of intestine descends through the femoral canal into the groin. B,Inguinal hernias are of two types. A direct hernia occurs through an area of weakness in the abdominal wall. In an indirect hernia, a loop of intestine descends through the inguinal canal, an opening in the abdominal wall for passage of the spermatic cord in males and a ligament of the uterus in females. (From Leonard PC: Building a medical vocabulary with Spanish translations, ed 9, St Louis, 2015, Saunders.)

FIG. 2.12 Example of flexible endoscopy. This endoscope is being used to examine the interior of the stomach through the esophagus. Depending on the structure to be examined, the physician chooses either a flexible or a rigid endoscope. Most of the interior stomach can be examined, including the antrum, located in the lower part of the stomach. (From Monahan FD, Neighbors M: Medical-surgical nursing: foundations for clinical practice, ed 2, Philadelphia, 1998, Saunders.)
Stomach Procedures
What parts of the anatomy are affected by these surgeries?
• Stomach
• Duodenum
• Vagus nerve
• Jejunum (in some cases)
• Vagus nerve (cranial nerve X)
Mapping
Check out the maps of five common gastric procedures:
Small Intestine Procedures
What parts of the anatomy are affected by these procedures?
• Stomach
• Duodenum
• Jejunum
• Ileum
• Cecum
Mapping
Let’s see how one procedure maps:
Large Intestine Procedures
See Fig. 2.13. What parts of the anatomy are affected by such procedures?
• Cecum

FIG. 2.13 Creation of an artificial opening in A, total colectomy and B, partial colectomy. (From LaFleur Brooks M, LaFleur Brooks D: Basic medical language, ed 5, St Louis, 2016, Elsevier.)

FIG. 2.14 Divisions of the large intestine. Illustration showing divisions of the large intestine and adjacent vascular structures. (From Patton KT, Thibodeau GA: Anatomy & physiology, ed 9, St Louis, 2016, Elsevier.)
• Transverse colon
• Descending colon
• Rectum
• Anus
Mapping
Let’s collect the information you’ll need to know about colectomy (Fig. 2.14), a surgery of the small intestine, and build a map:

Sigmoid and Rectal Procedures
What parts of the anatomy are affected by these procedures?
• Sigmoid
• Rectum
• Anus
• Large intestine
• Omentum
• Peritoneal covering of the mesentery
• Appendix
Mapping
Here’s the basic information you’ll need to know to assist at one procedure of the large intestine:
Anal Procedures
See Fig. 2.15. What parts of the anatomy may be affected by anal surgery?
• Sigmoid
• Rectum
• Anus
• Large intestine
• Omentum
• Peritoneal covering of the mesentery

Mapping
Here’s the map for one surgery of the anus.
Surgical Mapping
Hemorrhoidectomy
| Related Anatomy | Abnormal Anatomy | Pathology |
Sigmoid
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|