FIGURE 15-1 Twelve-lead ECG of patient’s atrial tachycardia on presentation to the laboratory. Deflections can be seen during the T waves in V1 suggesting 2:1 atrioventricular conduction.
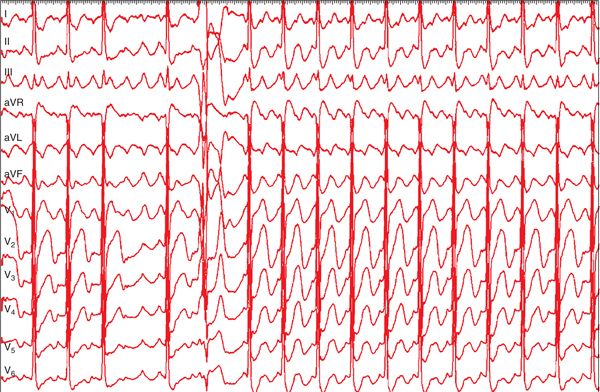
FIGURE 15-2 Surface lead electrocardiogram capturing a period of extended atrioventricular block during the tachycardia. The lack of an isoelectric component in several leads suggests a macroreentrant mechanism for this atrial tachycardia.
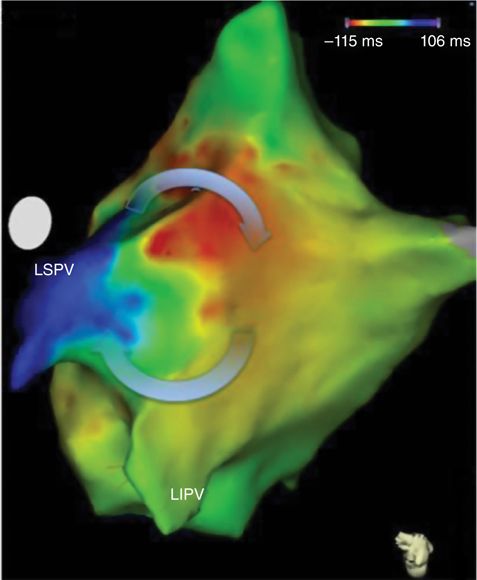
FIGURE 15-3 Activation map in the left atrium revealed a macroreentrant tachycardia through the previously ablated left pulmonary vein antra. Two conduction gaps around the left pulmonary vein antra, one near the roof and the other at the crux, facilitated the reentrant circuit. Note the “early meets late” activation point where the purple and red colors abut. LIPV = left inferior pulmonary vein; LSPV = left superior pulmonary vein.
Rapid atrial pacing at a slightly faster cycle length than the tachycardia cycle length (TCL) was performed at sites believed to be within the macroreentrant circuit. Pacing at the crux of the left superior pulmonary vein (LSPV) and left inferior pulmonary vein demonstrated a postpacing interval (PPI) minus TCL of 20 ms (Figure 15-4). At the junction of the left atrial roof and the LSPV, a multicomponent atrial electrogram was identified that displayed both near-field and far-field components. Rapid atrial pacing at this location revealed a PPI-TCL of zeroms for the near-field component and a PPI-TCL of –20 ms for the far-field component (Figure 15-5). Ablation at this site resulted in termination of the tachycardia (Figure 15-6) and rendered it noninducible.
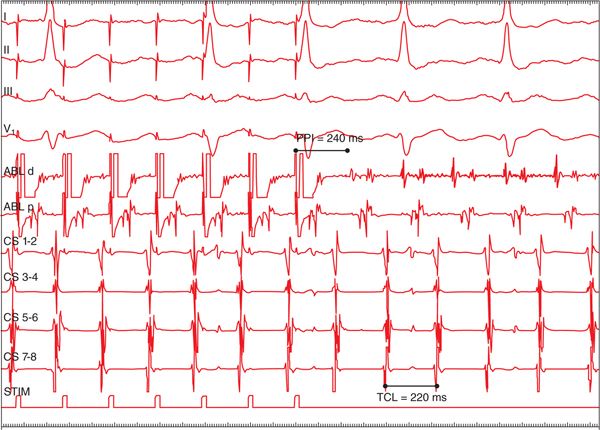
FIGURE 15-4 Rapid atrial pacing at the crux of the left superior and left inferior pulmonary veins revealed a postpacing interval (PPI) minus tachycardia cycle length (TCL) time of just 20 ms, indicating this location was at or very close to the tachycardia circuit. ABL = ablation; CS = coronary sinus; d = distal; p = proximal.
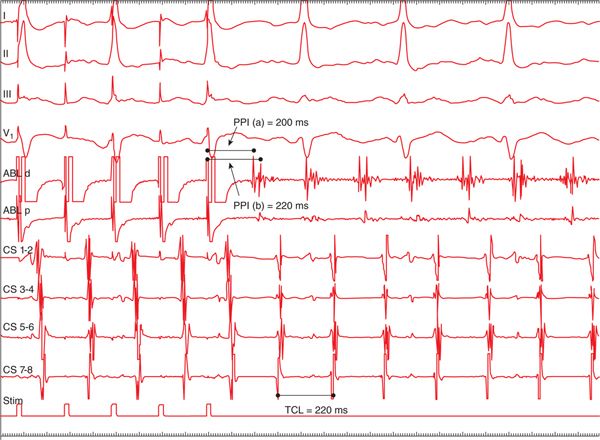
FIGURE 15-5 Rapid atrial pacing from the left atrial roof was performed during tachycardia. Note the multicomponent atrial electrogram at the distal ablation (ABL) catheter. The postpacing interval (PPI) to the initial component representing far-field atrial activity is actually 20 ms less than the tachycardia cycle length (TCL). The PPI to the second, or near-field component of the electrogram matches the TCL. CS = coronary sinus; d = distal; p = proximal.
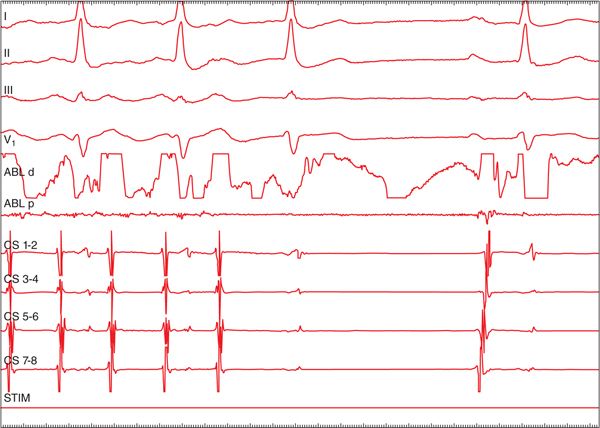
FIGURE 15-6 Termination of the atrial tachycardia to sinus rhythm during ablation at the junction of the left atrial roof and left superior pulmonary vein. ABL = ablation; CS = coronary sinus; d = distal, p = proximal.
FOCAL VERSUS MACROREENTRANT ATRIAL TACHYCARDIA
Classification of atrial tachycardia has evolved as diagnostic and therapeutic options for their management have evolved. Original classifications were based on mechanism (enhanced automaticity, triggered activity, and reentry) or appearance on surface ECG. More recently, atrial tachycardias have been classified as either focal or macroreentrant.1
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


