FIGURE 14-1 Patient’s presenting rhythm. The ablation catheter is positioned in the low right atrial septum, and a decapolar catheter is positioned in the coronary sinus (SC). Note the significant cycle length variability of the tachycardia with the septal atrial electrogram at times within the QRS complex. ABL = Ablation; d = distal; p = proximal; RVA = right ventricular apex; SC = coronary sinus.
Cycle length variability as great as 60 ms, as seen in Figure 14-1, is most commonly observed during atrial tachycardia. The occasionally simultaneous activation of the atria and ventricle ruled out orthodromic reciprocating tachycardia (ORT) as a sole diagnosis. Atrioventricular nodal reentrant tachycardia (AVNRT) with multiple slow pathways or multiple coexisting tachycardias could not be ruled out.
Ventricular pacing during the tachycardia revealed a V-A-V response (Figure 14-2). This response eliminates atrial tachycardia as the only mechanism of the tachycardia.1 The postpacing interval (PPI) in this tracing exceeded the tachycardia cycle length (TCL) by 100 msec, which is inconsistent with a diagnosis of AVNRT.2
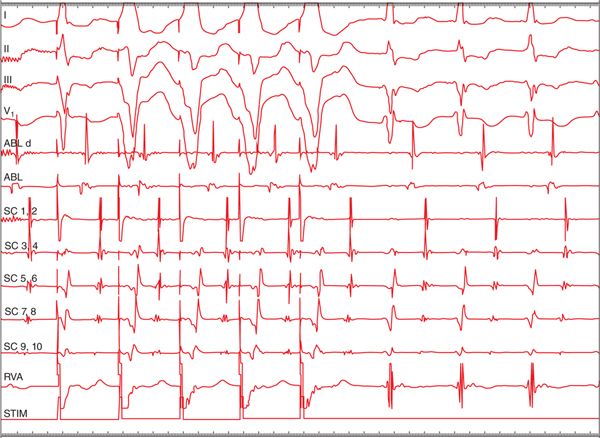
FIGURE 14-2 Entrainment of the tachycardia by ventricular pacing revealed a V-A-V response, consistent with either atrioventricular nodal reentrant tachycardia (AVNRT) or orthodromic reciprocating tachycardia. The postpacing interval minus the tachycardia cycle length was 100 ms, which is inconsistent with AVNRT. ABL = Ablation; d = distal; p = proximal; RVA = right ventricular apex; SC = coronary sinus.
Induction by atrial pacing (or spontaneous APDs) was not dependent on critical AH prolongation. Figure 14-3 shows an example of initiation with a single ventricular premature depolarization (VPD) with a V-A-A-V response. As is the case upon cessation of ventricular pacing that entrains a tachycardia, induction with a V-A-A-V response is indicative of an atrial tachycardia.

FIGURE 14-3 Tachycardia is initiated with a single ventricular premature depolarization. The method of induction is a V-A-A-V response, strongly indicating atrial tachycardia as the mechanism of the tachycardia. ABL = Ablation; d = distal; p = proximal; RVA = right ventricular apex; SC = coronary sinus.
A single tachycardia mechanism fails to adequately explain all of the findings previously described. The PPI <115 ms following ventricular entrainment made AVNRT unlikely. Initiation of the tachycardia with ventricular pacing followed by a V-A-A-V response as well as the significant tachycardia cycle length variability with lack of stability in the V-A interval confirms the presence of an atrial tachycardia. Entrainment with a V-A-V response with a relatively short PPI-TCL also suggests the presence of an accessory pathway and probable ORT.
Atrial activation mapping during the tachycardia demonstrated earliest atrial activation at the low right atrial septum. Ablation here terminated the tachycardia and rendered it noninducible. Following ablation, ventricular pacing demonstrated VA dissociation, indicating that both the atrial tachycardia and a posteroseptal accessory pathway were ablated at the same target site. The site of origin of the atrial tachycardia had been at or very close to the atrial insertion of the accessory pathway.
DIAGNOSING CONCEALED SEPTAL ACCESSORY PATHWAYS
Diagnosis of ORT utilizing a concealed septal accessory pathway is made based on tachycardia characteristics and pacing maneuvers during SVT. Differentiation of ORT from atypical AVNRT or in some cases focal atrial tachycardia can be challenging. Here, we describe techniques to differentiate these tachycardia mechanisms.
Para-Hisian pacing can be a valuable tool to confirm the presence of retrograde septal accessory pathway conduction as well as to verify successful septal accessory pathway ablation. The goal of para-Hisian pacing is to pace near the His bundle at high output and to gradually decrease the pacing output to produce complexes with right ventricular plus His capture and complexes with only right ventricular capture. When rapid retrograde conduction proceeds through an accessory pathway, similar conduction times
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


