Problem 43 An unwell young man in the emergency room
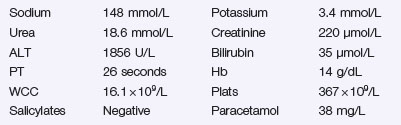
The following results become available:
Q.4
What are you going to do immediately? Describe and justify what you should look for on examination?
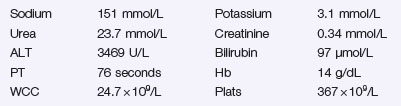
He is taken to the intensive care and intubated. Blood tests now reveal the following:
Answers
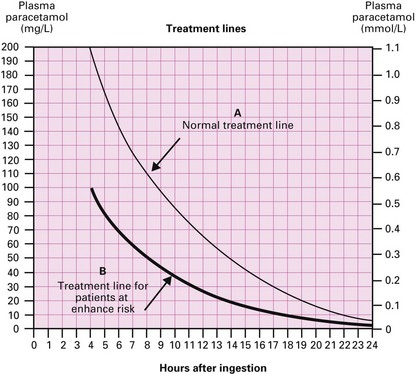
Figure 43.1 Paracetamol treatment chart.
(Courtesy of the Clinical Services Unit of the Royal Adelaide Hospital.)
All patients with deliberate self-poisoning should be assessed by psychiatric services.
A.4 This is a medical emergency.
A: Check and safeguard his airway
Call the anaesthetic team if his airway is threatened and he may need intubation.
The degree of unconsciousness should be determined by calculating and recording his Glasgow coma score (GCS), as shown in Table 43.1.
Table 43.1 The Glasgow coma score
| Eye Opening | Motor Response | Verbal Response |
|---|---|---|
| 4 Spontaneous | 6 Obeys commands | 5 Orientated |
| 3 To voice | 5 Localizes to pain | 4 Confused |
| 2 To pain | 4 Withdraws from pain | 3 Inappropriate words |
| 1 None | 3 Flexion to pain | 2 Incomprehensible sounds |
| 2 Extension to pain | 1 None | |
| 1 None |
The limbs should be tested for tone, response to painful stimuli and reflexes.



