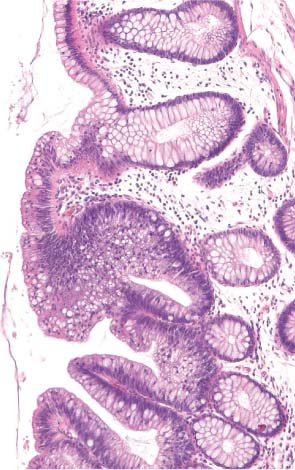
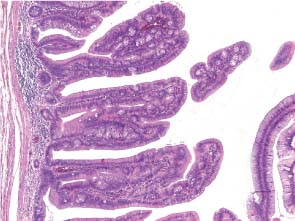
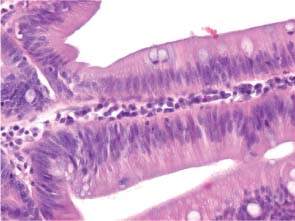
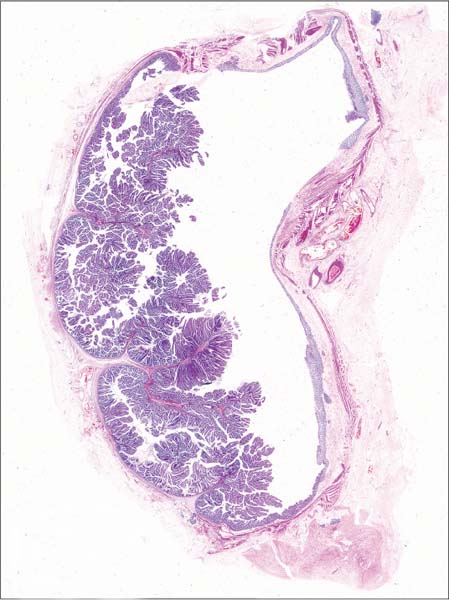
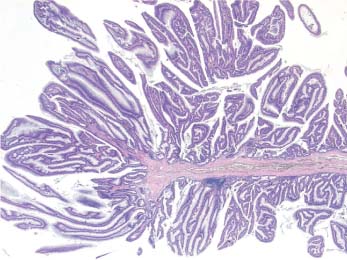
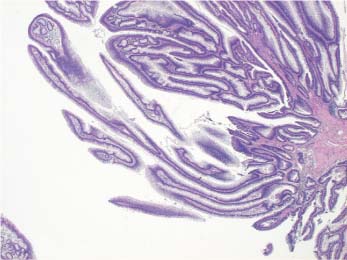
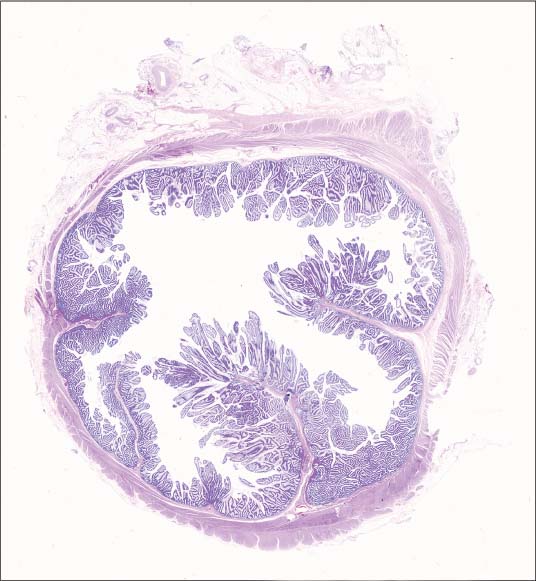
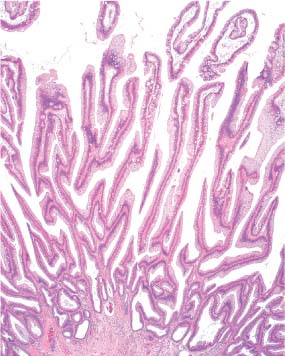
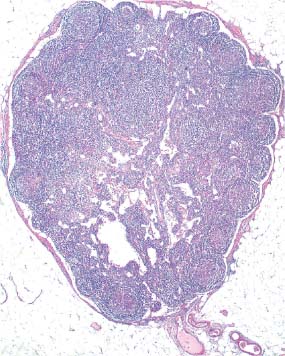
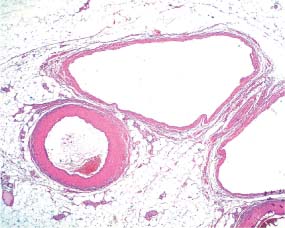
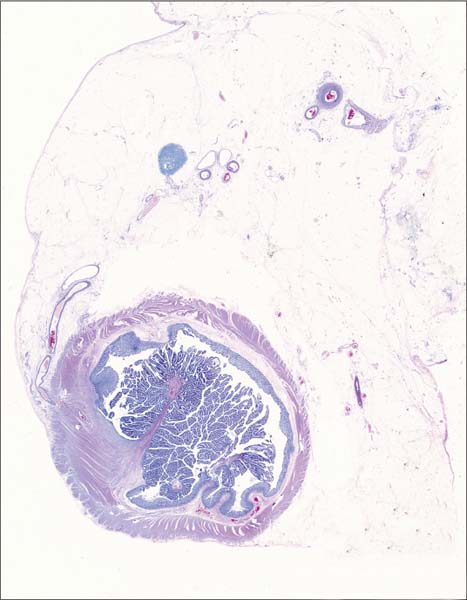
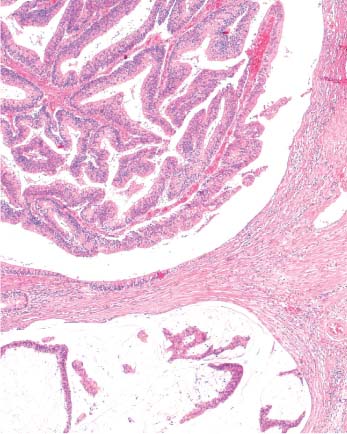
1 Adenomas Patient data: 63-year-old woman presenting with rectal bleeding. Endoscopically, a large, broad-based, soft and exophytic tumor was seen in her rectum, diagnosed on preoperative biopsy as adenoma. Surgical treatment: Rectosigmoidal resection, no preoperative irradiation. Specimen: 35-cm-long rectosigmoideum with an 8×6-cm soft exophytic tumor, 3 cm from the distal margin. Histopathologic diagnosis: Villous adenoma of the rectum with moderate dysplasia. No signs of severe dysplasia or invasion. Follow-up: 81 months, without signs of disease recurrence. Villous adenoma of the rectum is often a large non-pedunculated tumor, covering the rectal mucosa over an area of several centimeters. Endoscopic biopsies usually reach only the superficial part of the tumor, the delicate long villous structures covered by dysplastic epithelium. The large histologic section (Fig. 1.1) also demonstrates the intact lamina muscularis mucosae: no signs of invasion are present. It is easy to compare the structures of the normal bowel wall (indicated by the red arrow in the schematic image, Fig. 1.1d) to the structures of the adenoma (the left side of the image, green arrows in Fig. 1.1d). Adenomas exhibit a dysplastic epithelium. The transition from normal to dysplastic epithelium is illustrated in Figure 1.1a (corresponding to the area marked with a red rectangle in Fig. 1.1d). Figure 1.1b represents a microscopic image of the delicate villous structures of the adenoma (corresponding to the blue rectangle in Fig. 1.1d). Figure 1.1c is a magnified detail of Figure 1.1b, illustrating the moderately dysplastic epithelium of this adenoma exhibiting elongated, stratified and crowded cell nuclei and a reduced number of goblet cells. Fig. 1.1a Fig. 1.1b Fig. 1.1c Fig. 1.1 Large-section histology image of a villous adenoma of the rectum. Fig. 1.1d Schematic guide to the morphologic details in the large section in Fig. 1.1. Patient data: 84-year-old woman with intermittent rectal bleeding and a long history of recurrent adenomas in her rectum. Surgical treatment: Rectosigmoidal resection, no preoperative irradiation. Specimen: 33-cm-long rectosigmoideum with a 9-cm segment containing a circumferential exophytic tumor, 6 cm from the distal margin. Histopathologic diagnosis: Villous adenoma of the rectum with low-grade, partly moderate dysplasia. No signs of invasion. Follow-up: 6 months, without signs of disease recurrence. The large section in Figure 1.2 demonstrates another case of villous adenoma, which covers the entire circumference of the inner surface of the rectum. No signs of invasion are seen. The architecture of villous adenomas is complex, as they consist of primary finger-like processes extending outward from the bowel wall and containing fibromuscular stroma (indicated with blue arrows in Fig. 1.2c). Secondary finger-like processes, consisting of loose fibrous stroma with delicate vasculature and a surface covered by dysplastic epithelium, cover these structures. Figure 1.2a, b illustrate the complexity of these structures (corresponding to the red rectangle in the schematic image, Fig. 1.2c). Fig. 1.2a Fig. 1.2b Fig. 1.2 Large-section histology image of a villous adenoma of the rectum. Fig. 1.2c Schematic guide to the morphologic details in the large section in Fig. 1.2. Patient data: 55-year-old male examined for weight loss. Colonoscopy detected a polypoid lesion in the sigmoid colon, diagnosed as adenoma on preoperative biopsy. Surgical treatment: Sigmoidal resection, no preoperative irradiation. Specimen: 15-cm-long segment of the sigmoid colon containing a 3 × 3-cm exophytic tumor, 3 cm from the distal margin. Histopathologic diagnosis: Villous adenoma with moderate dysplasia. No signs of invasion. Follow-up: 31 months, no signs of disease recurrence. The patient developed prostate cancer 12months after the sigmoideum resection. The large section (Fig. 1.3) in the present case contains a transection of a villous adenoma of the sigmoid colon with long villous structures (magnified in Fig. 1.3a; the corresponding area is indicated by the yellow rectangle in Fig. 1.3d). Structures from the mesocolon are also seen in the same large section: a lymph node (indicated by the green arrow in Fig. 1.3d and magnified in Fig. 1.3b) and mesenterial blood vessels (indicated by the red rectangle in Fig. 1.3d and magnified in Fig. 1.3c). The large sections regularly include structures from the mesocolon, which is advantageous when assessing the extent of tumor growth. Fig. 1.3a Fig. 1.3b Fig. 1.3c Fig. 1.3 Large-section histology image of a villous adenoma of the sigmoid colon. Fig. 1.3d Schematic guide to the morphologic details in the large section in Fig. 1.3. Patient data: 88-year-old woman presenting with rectal bleeding. Endoscopically, an exophytic lesion was seen in her rectum. The preoperative endoscopic biopsy contained exclusively structures of adenoma. Surgical treatment: Rectosigmoidal resection, no preoperative irradiation. Specimen: 20-cm-long rectosigmoideum with a 6 ×5-cm exophytic tumor, 5 cm from the distal margin. Histopathologic diagnosis: Mucinous carcinoma, low grade, infiltrating in but not beyond the lamina muscularis propria, 23 lymph nodes without signs of metastasis, radical excision, mesorectal margin 20 mm. TNM stage: I (T2N0M0), Dukes A. Follow-up: 36 months, without signs of disease recurrence. Mucinous carcinoma may develop in villous adenomas. The large histologic section in Figure 1.4 demonstrates not only the mucinous carcinoma (green-colored area in the schematic image, Fig. 1.4c), but also the structures of the rests of the adenoma (orange arrows) as well as their relation to the cancer. To obtain a representative endoscopic biopsy, one has to reach the invasive part of the tumor, which is partly covered by the villous structures of the adenoma. Figure 1.4a, a microscopic magnification of the area indicated by the white rectangle in Figure 1.4c, shows the interface of the villous adenoma and the mucinous carcinoma. The large section offers proper documentation of the level of tumor invasion and, at the same time, reliably demonstrates the circumferential margin, including the mesorectal surgical resection margin. The mesorectal resection margin is easily assessed and its distance to the deepest invasive tumor structures is easy to measure, as indicated by the red double arrow in Figure 1.4c. The deepest level of invasion is indicated by the yellow rectangle in Figure 1.4c and is microscopically magnified in Figure 1.4b. Note also the four small reactive lymph nodes in the fatty tissue (encircled in Fig. 1.4c).
Case 1.1 Villous Adenoma of the Rectum
Practical points

Case 1.2 Villous Adenoma of the Rectum
Practical points

Case 1.3 Villous Adenoma of the Colon
Practical points

Case 1.4 Mucinous Carcinoma of the Rectum That Developed in a Villous Adenoma
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


