Chapter 10 Addiction and Abuse
Addiction can be described as occurring in cycles. The three general cycles include the following:
Scope of the Substance Abuse Problem
The statistics in Table 10-1 are from a 2007 survey in the United States by the Substance Abuse and Mental Health Services Administration and provide some information regarding the incidence of substance abuse.
TABLE 10-1 Survey by the U.S. Substance Abuse and Mental Health Services Administration (2007)
| Incidence of Substance Use | Number | Proportion of U.S. Population |
|---|---|---|
| Adults who will have engaged in nonmedical or illicit drug use at some time during their lifetime | 29 million | 15.6% |
| Adults who will develop substance dependence on illicit drugs during their lifetime | 5.4 million | 2.9% |
| People over the age of 12 who are current users of alcohol | 120 million | 51% |
| People over the age of 12 who met the criteria for alcohol dependence | 18 million | 7.7% |
| People aged 12 or older who were current (past month) users of a tobacco product | 70.9 million | 28.6% |
| People aged 12 or older who were current cigarette smokers | 60.1 million | 24.2% |
 Dependence: Physiologic condition whereby the absence of a drug results in withdrawal signs and symptoms. It is very closely related to the psychologic processes that occur with addiction, because the body and the mind are not completely separate entities (when you are physically unwell, you do not feel good), but strictly speaking, dependence refers to only the physical component of addiction.
Dependence: Physiologic condition whereby the absence of a drug results in withdrawal signs and symptoms. It is very closely related to the psychologic processes that occur with addiction, because the body and the mind are not completely separate entities (when you are physically unwell, you do not feel good), but strictly speaking, dependence refers to only the physical component of addiction.









Neurophysiology of Addiction
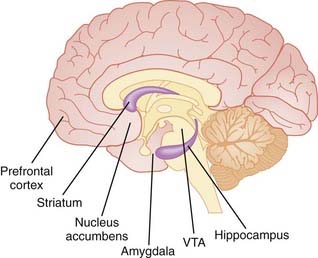
There are some important details related to neuroanatomy that are relevant to understanding the pathways of addiction; some of them include the following (Figure 10-1):
 Mesolimbic system: Pathway in the brain that projects from the ventral tegmental area (VTA) to the nucleus accumbens, amygdala, limbic system, and other areas of the brain. It is strongly implicated in addiction and dopamine processing.
Mesolimbic system: Pathway in the brain that projects from the ventral tegmental area (VTA) to the nucleus accumbens, amygdala, limbic system, and other areas of the brain. It is strongly implicated in addiction and dopamine processing.



Dopamine-Release Theory
 An example would be a mouse that learns to pull a lever to obtain food. The pulling of the lever leads to dopamine release, as the animal is predicting a reward, whereas the actual reward (food) does not elicit a response.
An example would be a mouse that learns to pull a lever to obtain food. The pulling of the lever leads to dopamine release, as the animal is predicting a reward, whereas the actual reward (food) does not elicit a response.
 Speed of onset is vital. A key distinguishing feature of an addictive substance is a rapid onset of action. This is why most of the substances listed in the following pages are delivered by routes that facilitate quick onset (i.e., intravenous, intranasal, inhalation). This also explains why heroin, which has a rapid onset of action, is considered to be one of the most addictive of opioids.
Speed of onset is vital. A key distinguishing feature of an addictive substance is a rapid onset of action. This is why most of the substances listed in the following pages are delivered by routes that facilitate quick onset (i.e., intravenous, intranasal, inhalation). This also explains why heroin, which has a rapid onset of action, is considered to be one of the most addictive of opioids.








