Acute Rheumatic Fever
Monica P. Revelo, MD, PhD
Dylan V. Miller, MD
Key Facts
Terminology
Acute, immunologically mediated, multisystemic inflammatory disease occurring a few weeks after an episode of pharyngeal infection with group A β-hemolytic Streptococcus, causing pancarditis
Clinical Issues
100 per 100,000 in developing countries
Heart failure, murmurs
Pericardial rub/effusion
Jones criteria
Major: Carditis (50%), migratory polyarthritis (most common), chorea (20%), erythema marginatum (5%), and subcutaneous nodules (3%)
Minor: Fever, arthralgias, previous rheumatic fever/rheumatic heart disease, prolonged PR interval in EKG, elevated sedimentation rate, and CRP
2 major or 1 major and 2 minor criteria and evidence of prior streptoccocal infection are needed for diagnosis
Macroscopic Features
Pericardium: Serofibrinous exudate (“bread and butter” pericarditis)
Endocardium: Valve swelling and small flat vegetations along closure line of mitral and aortic valve cusps
Microscopic Pathology
Myocardium with Aschoff nodules and nonspecific lymphocytic infiltrate
Valvular vegetations predominantly containing platelets
Pericardium with nonspecific inflammatory infiltrate
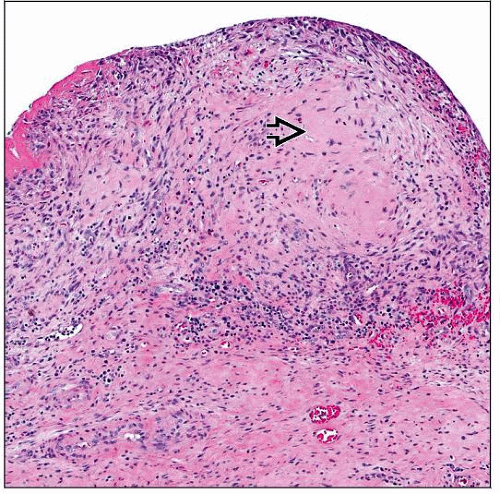 H&E stain of myocardial biopsy shows an Aschoff nodule with characteristic central eosinophilic connective tissue change  surrounded by mixed inflammatory infiltrate with numerous lymphocytes and histiocytes. surrounded by mixed inflammatory infiltrate with numerous lymphocytes and histiocytes. |
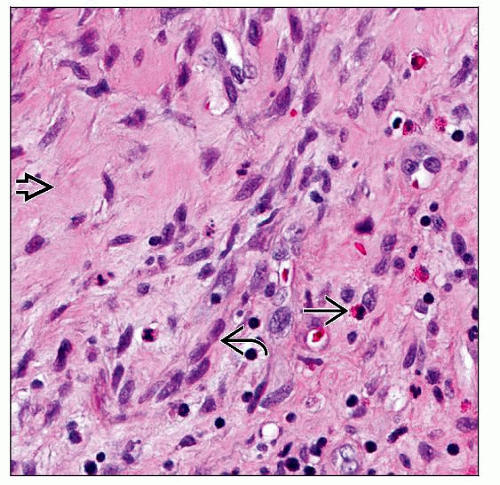 H&E stain of myocardial biopsy at higher magnification shows an Aschoff nodule with characteristic eosinophilic connective tissue change  surrounded by histiocytes surrounded by histiocytes  , lymphocytes, and eosinophils , lymphocytes, and eosinophils  . . |
TERMINOLOGY
Abbreviations
Acute rheumatic fever (ARF)
Definitions
Acute, immunologically mediated, multisystemic inflammatory disease occurring a few weeks after an episode of pharyngeal infection with group A β-hemolytic Streptococcus, causing pancarditis
ETIOLOGY/PATHOGENESIS
Infectious Agents
Heart injury is due to humoral and cellular immune-mediated reaction to streptococcal infection
Strains of M types 1, 3, 5, 6, and 18 are more rheumatogenic
Susceptibility to rheumatic fever has been linked to different HLA class II subtypes in different populations (DR 1, 2, 3, 4, 7)
Cross-reactivity between streptoccocal antigens and human heart tissue, particularly sarcolemmal membrane proteins and cardiac myosin, mediates tissue injury
CLINICAL ISSUES
Epidemiology
Incidence
100 per 100,000 in developing countries
< 2 per 100,000 in developed countries
Age
6-15 years
Gender
No predilection
Presentation
Heart
Heart failure
Arrhythmias and conduction abnormalities
Chest pain
Pericardial rub/effusion
New onset murmurs
Neurologic
Chorea
Skin
Erythema marginatum
Subcutaneous nodules
Joint
Arthralgias &/or polyarthritis
Systemic
Fever
Laboratory Tests
Elevated sedimentation rate
Elevated C-reactive protein (CRP)
Elevated antistreptococcal antibodies titre (ASO)
Throat swab culture positive for Streptococcus



