Above-Knee Amputation
Above-knee amputation is performed when it is not possible to save the knee joint because of the extent of injury or ischemic damage. Generally, the longer the stump, the better. The limiting factor is usually the condition of the skin and the soft tissues above the knee. If there is a question about the extent of gangrene or infection in the subcutaneous tissues in the skin, perform a guillotine amputation at the lowest possible level, leaving the stump open. When the infection is controlled, revise the amputation.
SCORE™, the Surgical Council on Resident Education, classified above knee amputation as an “ESSENTIAL UNCOMMON” procedure.
STEPS IN PROCEDURE
Symmetric fishmouth-type incision, preserving as much length as possible
Identify and ligate the greater saphenous vein
Divide muscles anteromedially to expose the femoral artery and vein
Suture-ligate and divide femoral artery and vein separately
Divide remaining muscles to expose femur
Use periosteal elevator to clean bone at site of division
Divide bone and smooth the ends
Ligate and divide profunda femoris artery and vein
Divide sciatic nerve and allow it to retract
Divide remaining muscles and soft tissues
Achieve meticulous hemostasis
Close in layers
HALLMARK ANATOMIC COMPLICATIONS
Recurrent ischemia
Neuroma
LIST OF STRUCTURES
Superficial fascia of the thigh
Fascia lata (deep fascia of the thigh)
Iliotibial tract
Lateral intermuscular septum
Anteromedial intermuscular septum
Posteromedial intermuscular septum
Femoral nerve
Obturator nerve
Sciatic nerve
Saphenous nerve
Femoral Vein
Greater saphenous vein (great saphenous vein)
Lesser saphenous vein (small saphenous vein)
Popliteal vein
Femoral Artery
Superficial femoral artery
Profunda femoris artery
Popliteal artery
Inferior Gluteal Artery
Ischiadic artery
Femur
Adductor (Hunter) canal
Adductor longus muscle
Adductor brevis muscle
Adductor magnus muscle
Gracilis muscle
Semimembranosus muscle
Semitendinosus muscle
Gluteus maximus muscle
Sartorius muscle
Tensor fascia lata muscle
Biceps femoris muscle
Quadriceps Femoris Muscle
Vastus lateralis muscle
Vastus medialis muscle
Vastus intermedius muscle
Rectus femoris muscle
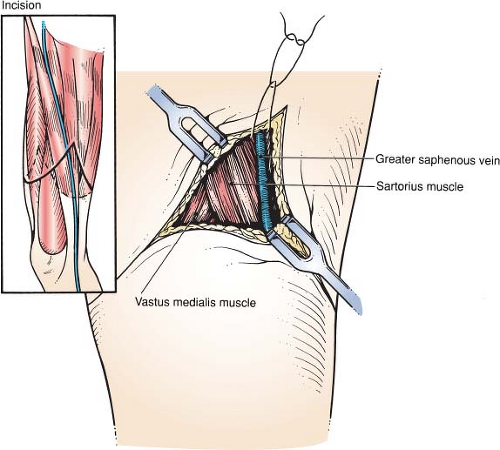 Figure 129.1 Position of the patient and development of flaps |
Position of the Patient and Development of Flaps (Fig. 129.1)
Technical Points
Position the patient supine with the leg draped free and allow the leg to fall into external rotation to facilitate access to the greater saphenous vein and underlying structures. Plan symmetric fishmouth skin flaps anteriorly and posteriorly. The flaps should be of approximately the same size and length. Gently curve the fishmouth to avoid interfering with the blood supply to the tip of the flap.
Make a skin incision and deepen the incision down to the fascia overlying the muscle groups. Identify and ligate the greater saphenous vein in the medial portion of the anterior flap. Incise the fascia sharply.
Anatomic Points
The greater saphenous vein and a variable number of tributaries are the only structures of consequence in the superficial fascia of the thigh. The course of the greater saphenous vein can be approximated by a line running from a point 8 to 10 cm posterior to the medial side of the patella to a second point that is level with, and 4 cm lateral to, the pubic tubercle. Note that, in the thigh, the larger veins of this system are in a plane between two layers of superficial fascia. Frequently, a large communicating branch between the lesser and greater saphenous veins ascends obliquely around the medial side of the thigh; other large tributaries join the greater saphenous vein on its anterolateral side. One fairly common variant of the greater saphenous system that would necessitate additional vein ligations is duplication of the greater saphenous vein in the more distal part of the thigh. When such duplication occurs, one of the vessels is typically deeper than the other, although both are still within the superficial fascia.
The deep fascia of the thigh, or fascia lata, is not of equal thickness throughout. It is thicker proximally and especially laterally, where it is reinforced by the iliotibial tract, which is actually the long, flat tendon of insertion (to the lateral condyle of the tibia) of the tensor fascia lata and most of the gluteus maximus. In addition, the fascia lata is thickened distally about the knee joint, where it is reinforced by fibrous expansions from the biceps femoris muscle laterally, the sartorius muscle medially, and the quadriceps femoris muscle anteriorly.
Division of the Anterior Muscles and Femoral Vessels (Fig. 129.2)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


