Problem 40 A middle-aged man with sudden visual loss
A 61-year-old man presents to the emergency department with complaints of sudden transient right monocular visual loss. During the interview, he gives a history of two such episodes over the past 24 hours, the last being just about an hour ago. During each episode, his vision became grey and washed out and cleared completely within 5–10 minutes. He denies other symptoms such as headache, nausea, ocular pain, redness, aura or visual haloes. You have been treating this patient for essential hypertension for approximately 5 years, although he has not been completely compliant with medication and follow-up for blood pressure monitoring. He has no other significant medical history, and his only medication is atenolol 50 mg daily. He is obese and is a habitual smoker. He is feeling physically fit, and you are unable to elicit any additional complaints in a review of symptoms. He has a bruit heard in the right neck.
On examination, you measure the blood pressure at 150/95 mmHg. There is no evidence of postural hypotension. Vision, visual fields, pupillary responses, anterior segment examination, gonioscopy and applanation tonometry findings are normal. Visualization of the retina with a direct ophthalmoscope reveals the finding illustrated in Figure 40.1.

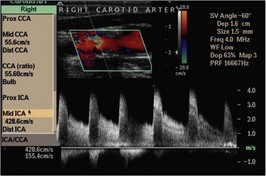
The patient decides in favour of the suggested surgical procedure. In preparation for this, the surgeon orders the radiological study illustrated in Figure 40.2.