Problem 9 A 63-year-old woman with a screen-detected abnormality
A 63-year-old woman underwent a screening mammogram which demonstrated an abnormal opacity in the left breast. There is no previous history of breast problems. Her sister was diagnosed with breast cancer at the age of 64 years 2 years previously. Current medications include combined oestrogen and progesterone hormone replacement therapy (HRT) that she has been taking for 12 years. Menarche was at the age of 10. She is married with two adult children aged 34 and 32 years.
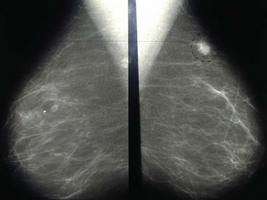
The mammogram is reviewed (Figure 9.1).
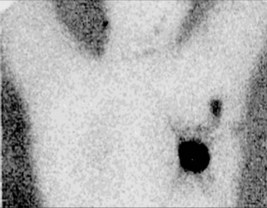
A surgical procedure is planned for the patient. The following investigation is performed immediately before the operation (Figure 9.2).
Answers
A.2 The following features on the mammogram would suggest malignancy:
The following features are more suggestive of a lesion being benign:
• A 2 cm dense, ill-defined solitary mass with spicules extending into the surrounding tissue in the upper outer quadrant.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


