Problem 23 A 59-year-old man with calf pain
A 59-year-old man presents with a 4-month history of pain in the right calf. The pain occurs only on walking and presents as a cramp-like discomfort, which comes on after he walks about 100 metres. The pain eases off when he stops walking, and he is still able to make his way to the local shops, although he is now reluctant to do so.
Q.1
What is the likely cause of his symptoms and what other information would you like from the history?
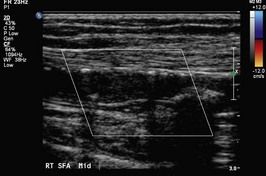
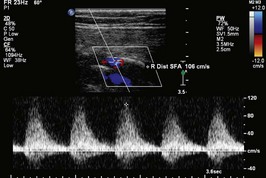
On your advice he agrees to see a vascular surgeon, who recommends that an arterial duplex scan is performed. This is shown in Figures 23.1, 23.2 and 23.3. Figure 23.2 demonstrates an occluded segment of superficial femoral artery (SFA). The waveforms above this lesion (23.1) are normal but the waveforms distally (23.3) are damped consistent with the occlusion just proximal to this segment. Subsequently he recommends a CT angiogram (shown in Figure 23.4). These are AP views with the patient’s right leg on the left side of Figure 23.1.