Problem 38 A 35-year-old woman with hypertension
A 35-year-old woman presents to the emergency department complaining of 5 days of progressive generalized headache and nausea. Her blood pressure is measured and is recorded at 250/140 mmHg. The patient states that she has a family history of hypertension and was noted to be hypertensive for the first time 2 years ago. She had no investigations, but was treated with verapamil 80 mg tds. The patient stopped taking this after a few months because it made her constipated.
On examination the patient is anxious and sweaty, but otherwise appears fit. Her pulse rate is 120 bpm and regular and her blood pressure 250/140 mmHg. Significant abnormalities include a forceful but undisplaced apical cardiac impulse without evidence of left ventricular failure, and a bruit in the left side of her abdomen. Urinalysis reveals 1+ (0.3 g/L) albumin only. Her retina is shown in Figure 38.1.
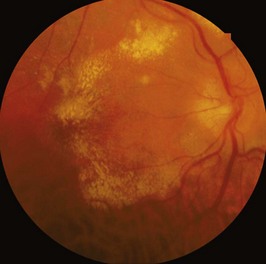
The changes seen on fundoscopy are consistent with the clinical picture of severe hypertension.
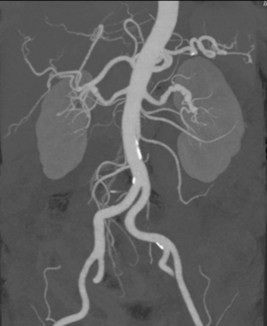
The patient went on to have the investigations shown in Figure 38.2 and Figure 38.3.

Answers
• Renal disease: thirst, polyuria, nocturia, dysuria, haematuria, colic, lethargy and general malaise of uraemia.
• Phaeochromocytoma: sweating, palpitations, anxiety and tremor, particularly occurring in paroxysms.
• Cushing’s syndrome: truncal weight gain, thinning of skin, easy bruising, weakness of proximal limb muscles, striae, hirsutism.
A.2 On examination you will need to look for evidence of hypertensive damage to:
• The retina (hypertensive retinopathy, especially haemorrhages, new exudates or optic disc swelling).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


