Problem 45 A 31-year-old woman with vertigo
A 31-year-old teacher presents to your general practice with a 2-day history of a sensation of the room spinning and unsteadiness while walking. The sensation is continuous and partially relieved by lying down. These symptoms have prevented her from going to work. She feels her hearing is normal and she has no tinnitus. Her only medication is the oral contraceptive pill.
Q.2
How do you differentiate central from peripheral causes of vertigo? What are some causes of each?
Q.3
How do you interpret this woman’s neurological signs?
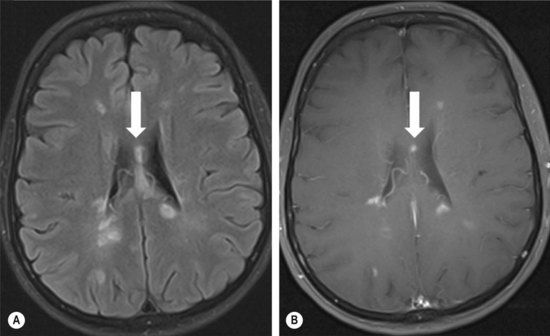
Given the probable site of the problem, the patient is referred to a neurologist. Her vertigo had improved but has not resolved completely. Various tests were performed. Figure 45.1A, B was taken from one of the tests.
Q.5
What is the likely diagnosis and what other tests could be done to further support the diagnosis?
Answers
You will also need to perform a careful general physical examination.
A.2 Signs suggesting central nervous system involvement include:
• Internuclear ophthalmoplegia (lateral gaze induces horizontal nystagmus in the abducting eye and incomplete or slowed adduction of the contralateral eye) – due to a lesion of the medial longitudinal fasciculus, which connects the abducens nucleus (CN VI) to the contralateral oculomotor nucleus (CN III).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


