CHAPTER 9 Back Pain: Neck, Upper Back, and Lower Back
INTRODUCTION
Statistics show that about 150 million Americans suffer from acute or chronic lower back pain and spend an estimated $20 billion to $50 billion a year in treating their problems.2 At any given time more than 2.6 million adults are disabled by chronic lower back pain. Reliable statistics as to how many Americans suffer from neck pain are not currently available, although one survey found that two thirds of the people surveyed had had significant neck pain at some time in their lives and 22% have neck pain that is bothersome.3
An interesting and disturbing study that appeared in 1994 in the New England Journal of Medicine found no direct correlation between structural abnormalities revealed on MRI and back pain: among 98 people without back pain, two thirds had spinal abnormalities, including herniated, bulging, or protruding intervertebral disks, disks with minor “degenerative joint changes,” and flattened narrowed disks, especially at the L5-S1 level.4 An investigation based solely on anatomic structure fails to produce an accurate diagnosis in 80% to 90% of patients with lower back disorders (LBD).5
BRIEF REVIEW OF THE NEUROMUSCULAR STRUCTURE AND SOFT TISSUES OF THE SPINE
This chapter presents a brief discussion of the neuromuscular system of the spine in order to assist acupuncture practitioners in understanding the possible underlying causes of back pain and to enable them to draw conclusions about the possibility of repairing the trauma. This information will help the practitioner to judge the likely therapeutic efficacy of acupuncture treatment for a given patient: whether acupuncture alone will be sufficient to achieve the desired result, whether the use of acupuncture by itself will be insufficient and other modalities should be involved, and whether the patient should be referred to other medical experts for further evaluation by means of X-rays, MRI, and so forth.
The entire spine (vertebral column) is made up of 34 bony vertebrae (Figure 9-1) and six additional elements: nerves, muscles, tendons, ligaments, disks, and various connective tissues. The erect spine consists of four physiologic curves: the cervical and lumbar lordosis (concave to the back) and the thoracic and sacral kyphosis (convex to the back). All of the four curves conform to the center of gravity.
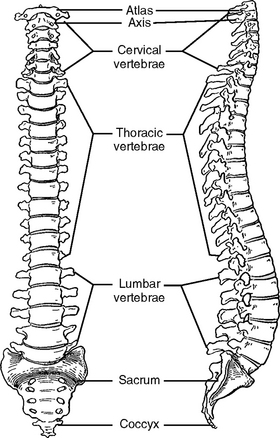
Figure 9-1 The vertebral column as a whole, anterior and lateral views.
(From Jenkins D: Hollinshead’s functional anatomy of the limbs and back, ed 8, Philadelphia, 2002, WB Saunders.)
Numerous types of neck and lower back pain are triggered by mechanical abnormalities or injuries, inflamed soft tissues, or degenerative diseases, and of course, the pain can be idiopathic, or “origin unknown.” Please note that the INMAS protocol (see Chapter 5) can be used successfully for pain management regardless of which underlying causes produce the pain symptoms as long as the symptoms are physiologically recoverable.
The Foundation of the Spine: The Coccyx and the Sacrum
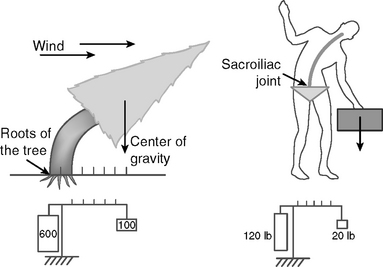
An analogy between the spine and a big tree will help to illustrate why many patients experience pain in this area. The trunk of a big tree (like the spine) has to support the canopy (the head) and numerous heavy branches (the upper limbs, ribs, and internal organs) that sprout from the trunk. This construction subjects the trunk to continuous mechanical stress and eventually the stress will affect the root system (the coccyx and sacrum bones).
The root system must be very strong and practically immovable to give adequate stability to the trunk and heavy branches of the tree. In calm weather, the tree ensures its symmetrical balance by having its branches spread in all directions and by evenly distributing gravitational stress among all the roots, which also spread in all directions. When a strong wind tilts the tree to one side, the symmetrical balance is lost and the roots from the opposite side of the tree sustain huge stress, which is many times higher than the weight of the tree (Figure 9-2). Using the physical principle of leverage, we can calculate the stress applied to the root system on the affected side of the tree. For example, if a tree weighs 500 pounds at its center of gravity, the affected part of the root system will sustain a stress of more than 5000 pounds.
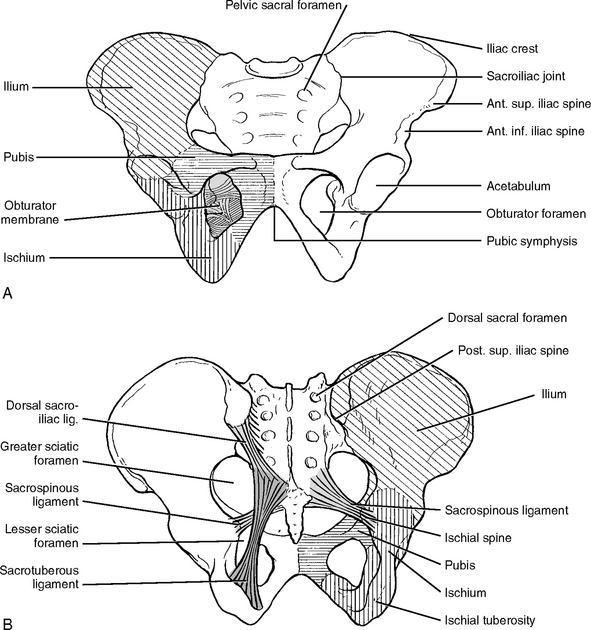
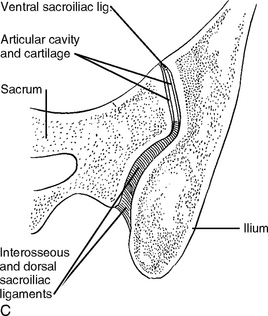
The sacroiliac (SI) joints differ from other joints. They are thicker and stronger and can move only a few millimeters (Figure 9-3). This relative immobility of SI joints stabilizes the spine against gravitational forces. The SI joints are also subject to the tremendous stresses and strains created by the forces of asymmetric imbalance as discussed in the above examples. The SI joints have to support the trunk, shoulders, arms, and head and to ensure a full range of motion.
INMAS is effective in treating painful symptoms related to the SI joint region. Most SI joint pain is caused by inflammation of the soft tissues such as nerves and ligaments. When needles are inserted into inflamed tissues, the needle-induced lesions break the blood vessels, thus stimulating the local defense immune reaction. As a result of the immune reaction, inflammation of the soft tissues of the SI joint is reduced. The needle-induced secretion of endorphins from the spinal cord and the brain reduces the physiological stress caused by the joint pain, thereby accelerating tissue healing. Eventually, this process restores normal SI joint function. The degree of recovery of SI joint function depends on the degree of the injury and the self-healing capability of the body.
The INMAS protocol for treating SI joints is provided at the end of this chapter.
Lumbar Spine (L1-L5)
The lumbar part of the spine is situated above the sacrum. The lumbar spine has five large vertebrae, and each vertebra has two upper facets (superior articular facets) that emerge from the top and two lower facets (inferior articular facets) that descend from the bottom (Figure 9-4).
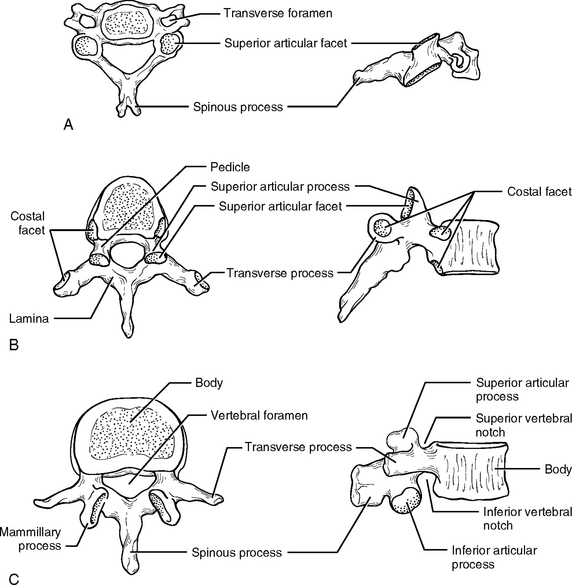
Thoracic Spine (T1-T12)
The two lower ribs are short and are called floating ribs. They do not enclose anything, but they allow a broader range of motion than the first 10 thoracic vertebrae. The joints between the last thoracic vertebra and the first lumbar vertebra (between T12 and L1) also facilitate side-to-side rotation of these relatively immobile regions. This rotation implies a significant amount of wear and tear on these lowest two thoracic vertebrae and may result in various pain syndromes and degenerative diseases like osteoarthritis.
Cervical Spine
The cervical spine has seven vertebrae. These vertebrae get progressively smaller as they approach the bottom of the skull (see Figure 9-4). The cervical spine is the upper part of the spine and is capable of a great range of motion, in contrast to the foundation of the spine, the sacrum and coccyx, which has fused bones and almost immovable sacroiliac joints. For instance, the cervical spine allows the neck to turn 90 degrees in either direction, the ear to almost touch the shoulder, and the head to lean backwards more than 70 degrees.
The cervical spine is composed of two major complexes: the upper cervical segment (C1 and C2) and the lower cervical segment (C3 to C7). The occipital bone of the skull sits on the ring-shaped bone C1, which is called the atlas. The joint between them (0-C1), which is the first joint of the cervical spine, is called the atlantooccipital (AO) joint. This joint provides a very important function by anchoring the skull to the spine, and it is therefore necessarily the most immobile joint of the neck spine.
The distinctive feature of C2 is a blunt toothlike process called the odontoid process, or dens, projecting superiorly from the body (Figure 9-5). C1 uses the dens of C2 as its pivot for rotation. The front inner surface of the ring-shaped C1 is attached to the dens of C2, allowing C1 with the skull on top of it to rotate against the dens.
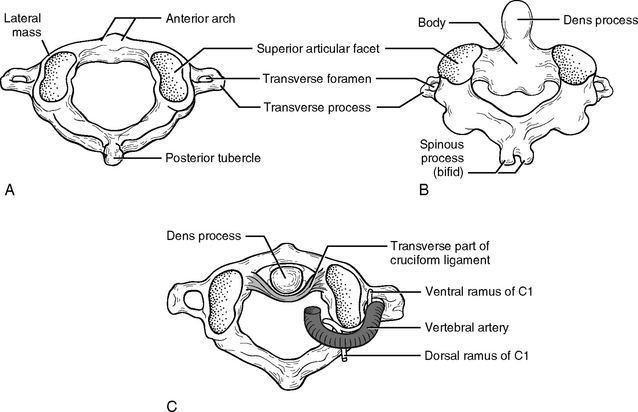
Figure 9-5 Posterosuperior views of the atlas (A) and axis (B). C, Superior view of the atlantoaxial joint.
(From Jenkins D: Hollinshead’s functional anatomy of the limbs and back, ed 8, Philadelphia, 2002, WB Saunders.)
The peripheral nerve network in the neck region is some of the most complicated nervous wiring in the body. Eight cervical nerves emerge from the intervertebral foramen to form the cervical plexus from C1 to C4, and brachial plexus from C5 to T1. The intervertebral foramen is the passage from which the spinal nerve emerges. The neck is also the passage for the autonomic nervous system, which balances the physiological activities of the majority of the internal organs. Thus, pathological neck problems will affect not only the head and the arms but many different organs ranging from the brain to the large intestine.
During a whiplash accident, the horizontal force from the back causes the neck to overextend and overflex (Figure 9-6), which causes damage to both posterior and anterior joints. In addition, the translational back-and-forward movement of the upper vertebra closes the vertebral canal, which causes injury to the spinal cord. Understanding the basic mechanical structure of the spine and the nature of pathological damage sustained by the spine during an accident is the key to effective acupuncture treatment for back pain.
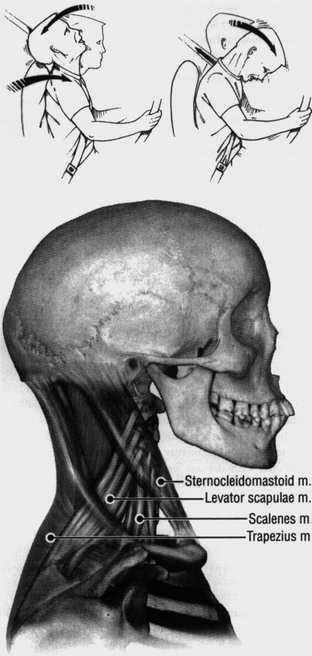
Figure 9-6 Overextension and overflexion during a “whiplash” injury.
(From Wall P, Melzack R: Textbook of pain, ed 4, Edinburgh, 1999, Churchill Livingstone.)
The INMAS protocol for treating whiplash will be provided in the end of this chapter. Please note that in the case of whiplash, pain symptoms such as neck pain, lower back pain, and upper back pain are all closely related because functionally and anatomically all three parts of the spine—the neck, the upper back, and the lower back—are interrelated structures that should be understood as one whole entity and treated as such.
MUSCLE
Muscles perform at least three major mechanical functions:
Weak back muscles are not able to adequately perform the following functions:
Usually a spasm has no serious consequence and the pathological effect is not longlasting. However, when a tear caused by strain or spasm is severe or repeated, scar tissue is formed, which weakens the muscles and irritates the nerves, thus provoking pain syndromes. Acupuncture needling is very effective in the treatment of strained tissues and muscle spasms, especially at the acute phase.
Weak abdominal muscles often result in back pain. The abdominal muscles do much of the work when lifting or carrying loads, and so when weak abdominal muscles try to relieve the strain on back muscles during such activities, they will sustain further damage. This is why the abdominal muscles should be examined and needled in clinical acupuncture practice when a patient presents with back pain.
The Shortened Muscle Syndrome
The paraspinal muscles, when shortened, draw two adjacent vertebrae closer together, which narrows the intervertebral space and foramen (Figure 9-7). The results are a bulging disk and a compressed nerve root. A vicious circle is gradually built up: shortened muscles cause compressed nerve roots (radiculopathy), and compressed nerve roots lead to further muscle shortening.4
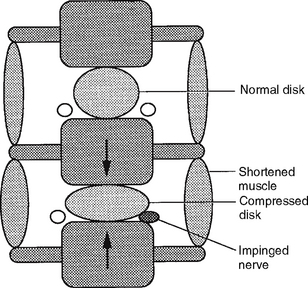
Figure 9-7 Shortened paraspinal muscles across an intervertebral space compress the disk and nerve root.
(From Filshie J, White A: Medical acupuncture: a Western scientific approach, Edinburgh, 1998, Churchill Livingstone.)
Acupuncture treatments can break this vicious circle by using needles to produce a minimal tissue injury, which stimulates the relaxation of muscle stress. The primary goal in the treatment of muscle shortening is relaxation of the affected muscle, and acupuncture needling achieves this goal more swiftly and precisely than any other medical modality. When a fine acupuncture needle pierces a muscle, it pushes aside tissue, disrupts the cell membrane, and inflicts a minute tissue injury, which mechanically creates a brief outburst of microcurrents (injury potentials). The microinjury that results from needling generates relatively longlasting currents that stimulate the mechanism of repair and regeneration of the affected tissue (see Chapter 3). Thus, acupuncture treatment eliminates the pathological condition responsible for muscle shortening. After treatment a patient feels either no pain or a significant alleviation of pain.
NERVE TISSUE
Injury to nerves leads either to an involuntary, intense contraction (spasm) of the muscles in the body, the blood vessels, and organs, or to weakness or paralysis of the muscles as a result of insufficient contraction. A spasm causes overstimulation of sensory nerves and undernourishment of muscles because the tightness constricts blood vessels and interrupts the mechanism of nourishment. Weak muscles can easily be overstretched and thus be susceptible to painful tissue damage because this pathological overstretching releases chemicals that irritate the muscles (Chapter 3). Some of the pathophysiologic conditions of the spinal cord are discussed below.
Spinal Stenosis
Lumbar spinal stenosis is defined as a condition involving any type of narrowing of the spinal canal, nerve root canal, or tunnels of intervertebral foramina.5 Spinal stenosis can be either congenital or acquired. Acquired stenosis may be due to degenerative conditions (spondylolisthesis, see below), failed medical procedures (postlaminectomy, postfusion, postchemonucleolysis), or posttraumatic injuries, or it may be secondary to disk herniation (see below). Narrowing can occur in one or several locations of the same vertebral segment or it can affect several segments. The canal space can be narrowed by pathological changes in the soft tissues, scar tissue, or bony tissue impingement (bone spurs). Severe stenosis results in nerve compression. Soft tissue encroachment or abnormal bone growth such as osteophyte formation reduces the size of the intervertebral foramen and causes foraminal stenosis.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


