CASE 61
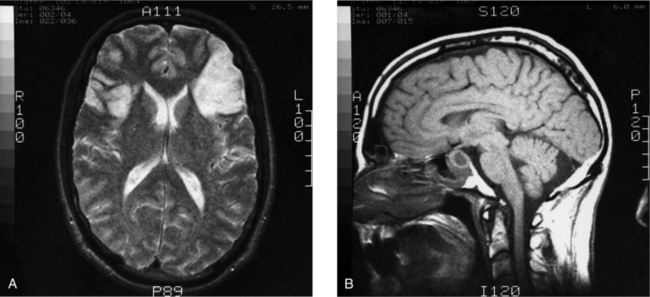
A 55-year-old man was found in a closed garage with the car engine running. Police initially concluded it was a suicide attempt. He was treated for carbon monoxide poisoning. Upon questioning of his family, it was learned that everything had gone well over the holidays and everyone in the family was fine. He really had no reason to kill himself and had never discussed it. Further questioning of his family revealed certain behavioral changes to include forgetfulness and mild confusion, and complaints of headaches. A neurologic examination of cranial nerve function indicated extraocular muscle movements were limited. A magnetic resonance imaging (MRI) study was ordered. Results of the MRI showed bilateral watershed infarcts of the frontal lobes caused by a pituitary gland tumor (Fig. 7-35).
WHAT IS THE EMBRYOLOGIC ORIGIN OF THE PITUITARY GLAND?
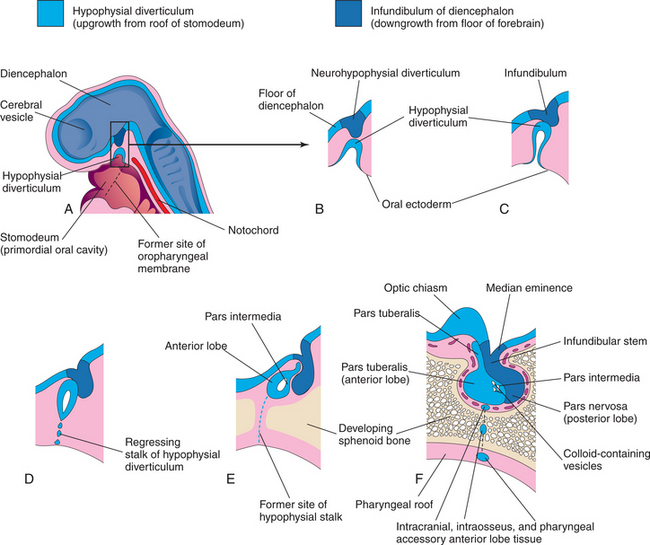
The distinct histologic differences of the adenohypophysis and the neurohypophysis are explained by their dual embryologic origin (Fig. 7-36). The neurohypophysis, being composed of neural elements, is derived from the neuroectoderm of the diencephalon. The adenohypophysis, being glandular in nature, has an epithelial origin from the ectoderm lining the roof of the stomodeum (primitive mouth). A diverticulum, called the hypophysial (Rathke’s) pouch, develops from the oral ectoderm, ultimately giving rise to the adenohypophysis.
SURGERY IS THE PREFERRED PROCEDURE FOR TREATING TUMORS OF THE PITUITARY GLAND. ONE METHOD OF ACCESSING THE GLAND IS BY ENTERING THE NOSTRIL. HOW IS THIS ANATOMICALLY POSSIBLE?
A transsphenoidal surgical approach is practical because of the anatomical relationships (remember, to know your anatomy is to know your anatomical neighbors!) of the pituitary gland, sphenoid sinus, and nasal cavity. Surgical instruments are inserted into the right nostril and passed along the superior margin of the nasal septum (Fig. 7-37
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


