CHAPTER 6. VENEPUNCTURE (PERIPHERAL AND FEMORAL)
Indications54
Contraindications54
Peripheral venepuncture equipment54
Practical procedure55
Femoral venepuncture equipment58
Practical procedure59
Post-procedure investigations61
Complications61
Venesection is probably the oldest surgical intervention. It was used therapeutically by Hippocrates (460–377 BC), while Aulus Cornelius Celsus (25 BC–AD 50) gave it a scientific context and described the technique in De Re Medicina. It became a universal remedy in virtually all cultures. It had spectacular results in those with pulmonary oedema secondary to rheumatic heart disease but was less successful in those with asthma, convulsions, etc., where it was equally applied and consequently was the source of controversy as a universal remedy. In Graeco-Arabic medicine (Unani) it was thought to let out putrid humours. This concept was later supplemented by the practice of blood fortification by the administration of iron-containing substances. Such practice persisted well into the 19th century in the western world. Today venesection is largely for investigative rather than therapeutic purposes.
INTRODUCTION
Phlebotomy or venepuncture is a basic clinical skill that is routinely practised by a number of health professionals. Peripheral venepuncture should be performed efficiently with minimal discomfort to the patient. Occasionally peripheral venepuncture may be difficult or contraindicated and femoral venepuncture is indicated.
INDICATIONS
• Routine blood investigations: haematology; biochemistry; immunology.
• Transfusion samples: group and cross-match/group and save.
• Toxicology samples: therapeutic drug monitoring (e.g. gentamicin, vancomycin, phenytoin levels); assays in overdose (e.g. paracetamol).
• Microbiology investigations: blood cultures (covered in a later chapter); serology.
CONTRAINDICATIONS
• Local infection.
• Superficial or deep venous thrombosis.
• Ipsilateral mastectomy, (i.e. a limb with impaired lymphatic drainage).
• Ipsilateral hemiparesis or contractures.
• Ipsilateral arterio-venous fistula.
• Lack of consent.
PERIPHERAL VENEPUNCTURE EQUIPMENT
• Vacutainer® needle or Monovette® needle.
• Vacutainer® barrel or Monovette® attachment.
• Sterile alcohol swabs.

• Cotton wool balls.
• Plaster.
• Tourniquet.
PRACTICAL PROCEDURE
• Explain the procedure to the patient and gain consent.
• Break the paper seal and twist the Vacutainer needle into the barrel.
• Place the arm on a comfortable surface such as a pillow.
• Place tourniquet on the upper arm sufficiently tight to distend veins but not occlude the artery (check the pulse is palpable below the tourniquet).
• Look and feel for a vein, noting the size and direction of the vein (Fig. 6.3). Start in the antecubital fossa and work your way down the arm. Aim to select a vein that has not been used recently for venepuncture, is easily located, feels bouncy and refills quickly when pressure is applied.
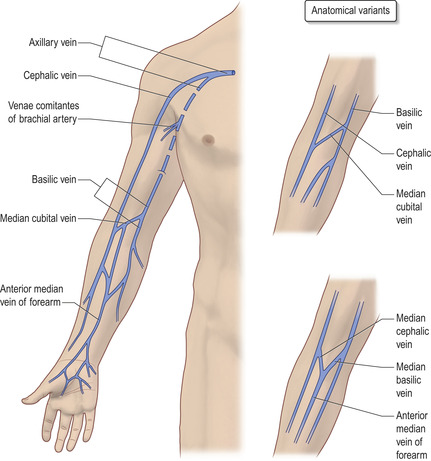 |
Fig. 6.3 Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|