CHAPTER 6 Quantitative Acupuncture Evaluation and Clinical Techniques
INTRODUCTION: QUANTITATIVE EVALUATION PREDICTS THE EFFICACY OF ACUPUNCTURE THERAPY
The following clinical example can help us to understand the nature of acupuncture therapy.
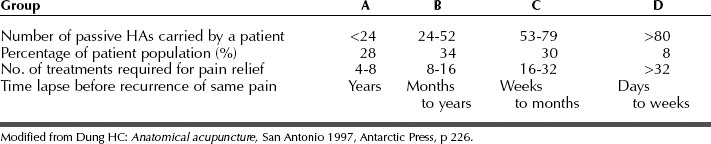
Statistically, patient A represents 28% of the patient population who can completely self-heal; patient B, 34%; patient C, 30% (B and C can partially self-heal); and patient D, 8% (can slowly, or not all, self-heal) (Table 6-1).
QUANTITATIVE ACUPUNCTURE EVALUATION
Thus the number of tender homeostatic acupoints (NHAs; see Chapter 5) shows the interaction between the self-healing potential (HP) and the severity of the symptoms (SS). This relationship can be roughly expressed in the following linear formula:

Dr. H.C. Dung classified patients into four groups (see Table 6-1) according to their self-healing potential and treatment prognosis, after studying more than 15,000 cases.
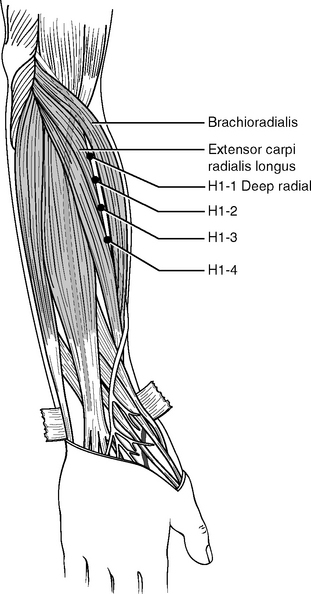
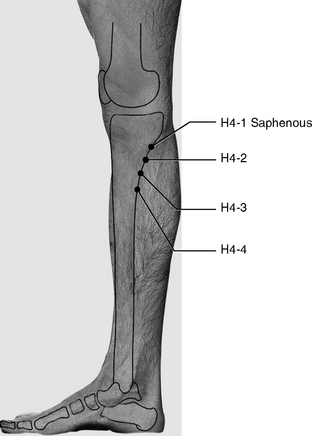
The selected landmark acupoints for patient evaluation are the H1 deep radial on the forearm (Figures 6-1 and 6-2) and H4 saphenous (Figure 6-3). The deep radial nerve and the saphenous nerve are similar to one another. Both emerge from deep tissues at similar locations just below the elbow and knee and start to branch to innervate other muscles. Figures 6-1 and 6-3 show that more HAs can appear distally to both H1 and H4. These additional points are located along the deep radial and saphenous nerves, about 2 to 3 cm apart. We call these points H1-2, H1-3, H1-4 (located on the deep radial nerve) and H4-2, H4-3, H4-4 (located on the saphenous nerve). Thus the total number of points is 16 bilaterally.

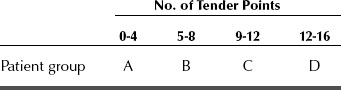
When examining a patient we palpate all these 16 diagnostic points on the forearms and legs on both sides of the body. Using the results of this examination we can classify our patients into four groups, as shown in Table 6-2.
Table 6-2 Classification of Patients According to 16 Evaluation Points (H1−1, −2, −3, −4) + (H4−1, −2, −3, −4)
By combining data from Tables 6-1 and 6-2, we can predict the efficacy, duration, and outcome of acupuncture treatments. Statistical analysis shows that about one third of patients belong to group A (28%). The effects of acupuncture can seem miraculous for this group. Group D accounts for about one tenth of patients (8%), and these are least able to benefit from acupuncture therapy. Most patients, about 64%, belong to groups B and C and represent an average or slightly below average health level. Acupuncture treatments can successfully control chronic pain for patients in groups B and C for some time. In some cases the pain will recur in about 4 to 6 months (see Table 6-1); some patients may enjoy longer pain relief if they take appropriate measures for health maintenance. The mechanism of pain relapse was explained in Chapters 3 and 5. Age and genetic factors may influence the self-healing potential. The age of most group A patients is below 40, and most group D patients are above 60 years of age. Nevertheless it is not uncommon to see older patients in group A and younger patients in group D. We should not assume that older patients are necessarily sick or weak.
The following simple guidelines facilitate the evaluation procedure:
CLINICAL TECHNIQUES
Definition of Efficacy of Acupuncture Treatments
Acupuncture efficacy is measured by (1) the number of treatments needed for maximal relief and (2) the duration of the pain relief. It depends on the interaction between a patient’s self-healing potential and the severity and nature of the symptoms. In Tables 6-1 and 6-2, we classify pain patients into four groups: A, B, C, and D. Accordingly we can classify acupuncture efficacy into four groups: excellent for group A, good for group B, average for group C, and poor for group D. Different groups need a different number of treatments and experience different durations of pain relief.
Collecting Information to Evaluate a Patient’s Healing Potential
Medical History
It is important to collect precise information about any surgical procedures the patient has undergone. Pain symptoms can be more difficult and time consuming to treat when they persist after surgery. This is because surgery alters some of the neuroanatomic structure, whereas acupuncture works best when applied to intact body anatomy.
Syncope or “Needle Fainting”
Dr. Chen, of the Center for Traditional Chinese Medicine of Veterans General Hospital in Taipei, Taiwan, reported 55 syncope events in 28,285 clinical acupuncture visits (0.19%).1 These data are similar to our own clinical evidence. According to Dr. Chen’s statistical analysis, 28,285 visits account for about 3,235 patients, with each patient having an average of eight acupuncture treatments. Thus an acupuncture practitioner may encounter one syncope event in about every 500 treatments; in other words about 2% of patients in an acupuncture clinic will experience syncope. Fortunately syncope, or “needle fainting” as it is called in China, can be predicted and prevented.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


