CASE 47
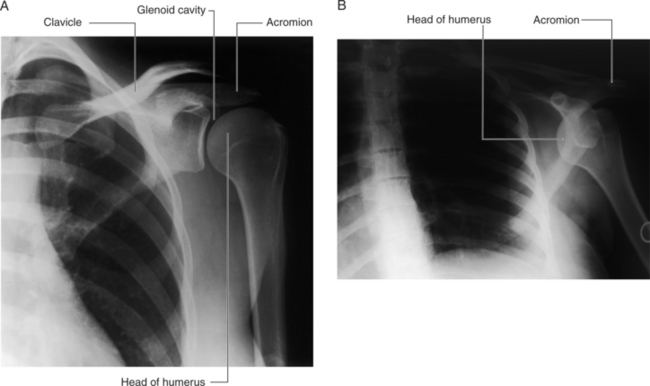
During a college football game, the 21-year-old right-handed quarterback preparing to pass the football was tackled from behind by the opposing linebacker. As he was tackled, the quarterback’s abducted left arm was driven into the turf. After the tackle, the quarterback was in excruciating pain and was unable to move his left arm at the shoulder joint. He was transported to the affiliated University Medical Center for medical care. During his physical examination, the physician noted that the patient’s left arm was slightly abducted and was laterally (externally) rotated and the range of motion was limited. The doctor also was able to palpate the left humeral head. A neurologic examination revealed paralysis of the deltoid muscle and a loss of skin sensation over the central area of the deltoid. A series of radiographs confirmed the diagnosis of dislocation of the glenohumeral joint (Fig. 6-13) and a MRI study showed a Bankart’s lesion. The dislocation was reduced and the Bankart’s lesion was surgically repaired.
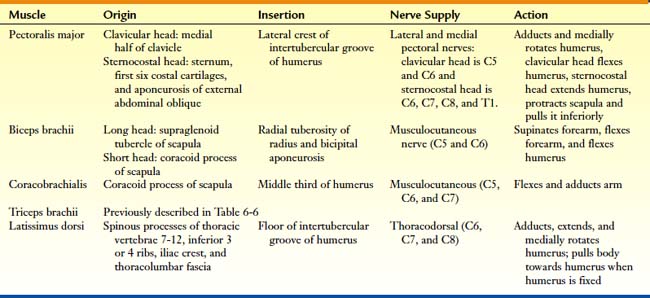
BESIDES THE DELTOID, TERES MAJOR, AND ROTATOR CUFF MUSCLES, WHAT OTHER MUSCLES ACT ACROSS THE SHOULDER JOINT?
The additional muscles and their attachments, innervation, and actions that act across the shoulder joint are described in Table 6-11.
WHAT ARE THE FUNCTIONAL AND ANATOMICAL CLASSIFICATIONS OF THE GLENOHUMERAL JOINT?
The fibrous capsule of the joint extends from the margin of the glenoid cavity to the anatomical neck of the humerus. The joint is reinforced anteriorly and superiorly by intrinsic ligaments and anteriorly, superiorly, and posteriorly by the rotator cuff muscles. Because the inferior portion of the fibrous capsule is not strengthened, this represents its weakest point.
The intrinsic ligaments of the joint are the (Fig. 6-14):
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


