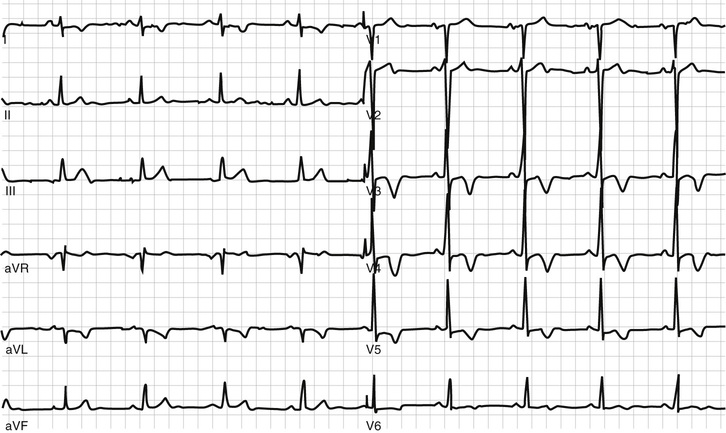
Brandon A. Miller Approximately 1 to 2% of primary care visits are for chest pain, and it is always important to consider a cardiac etiology given that heart disease is the number one cause of death in the United States. It is also important to keep in mind that the majority of outpatient visits for chest pain involve noncardiac etiologies, with approximately 36% of cases involving a musculoskeletal condition, 19% involving a gastrointestinal condition, 8% involving a psychosocial or psychiatric condition, 5% involving a pulmonary condition, and 16% involving nonspecific chest pain (or chest pain of unclear etiology). This leaves about 16% of cases with a serious cardiac etiology, either stable coronary artery disease (angina in about 10% of cases) or unstable coronary artery disease (unstable angina, pulmonary embolism, heart failure comprising the other 6%). Compare this to the approximately 50% of patients in the emergency department setting that present with chest pain from serious cardiovascular etiology (either acute coronary syndrome, stable angina, pulmonary embolism, heart failure, or aortic dissection). The patient has several risk factors for coronary disease, including hypertension, prediabetes, hypercholesterolemia, a significant smoking history, and a family history of coronary artery disease. Given the patient’s underlying risk, you should hold a high level of suspicion for heart disease. The patient has many symptoms of typical (or classic) angina, including a midsternal location, a squeezing quality, a relatively predictable onset with exertion, a duration lasting between 2 and 15 minutes (usually 2 to 5) with a crescendo–decrescendo pattern and abatement with rest. If he had been prescribed sublingual nitroglycerin in the past for his symptoms and this resulted in relief, this is also a typical feature. Although the patient has many typical features, there are other features of stable angina that he doesn’t have but that are worth noting. These include a description of the discomfort as a heaviness, burning, pressure, weight, or ache (typical cardiac discomfort is rarely described as an outright pain). Although the onset of pain is usually with exertion, it can occur with emotion (frustration, anger, sadness) or eating a large meal (due to a “steal-like” phenomenon as blood is diverted to the gastrointestinal [GI] tract to aid in digestion). The discomfort can also radiate, usually to the shoulders, neck, jaw, inner arm (can be down to the ulnar forearm), lower chest, or back. Discomfort associated with coronary artery disease is rarely located below the umbilicus or above the jaw. It is also important to understand that there also exists a category of atypical symptoms that can be associated with stable coronary artery disease. These should be considered in elderly patients, women, and diabetics and are known as “anginal equivalents.” Patients may describe fatigue, nausea, dyspnea, lightheadedness, and diaphoresis that occur with exertion or strong emotions. Patients who describe their pain as pleuritic, sharp, pricking, stabbing, or choking are less likely to have coronary artery disease as the etiology for their pain. Similarly, those who describe their pain as either originating in the inframammary region, lasting for only seconds, or made worse with palpation are not likely to have an underlying cardiac etiology. Given the patient’s typical anginal symptoms, the stability of the symptoms over time, his lack of chest pain at this visit, and his underlying risk factors for coronary artery disease, you give a diagnosis of stable angina from coronary artery disease until proven otherwise. Stable angina refers to the symptoms patients have when they have atherosclerotic plaques in the coronary arteries that obstruct blood flow, resulting in regional myocardial ischemia occurring during times of increased myocardial oxygen demand (usually exertion or emotional stressors that cause tachycardia). The severity of the symptoms does not correlate with the severity of coronary artery disease seen on cardiac catheterization, and one or more vessels can be involved with any degree of symptoms. Usually, an epicardial coronary artery needs to be at least 70% stenosed to cause symptoms. The patient is sent to another room for his ECG and returns. Your interpretation of the ECG is as follows: normal sinus rhythm with a rate of 76/min, no significant Q-waves are present, normal PR and QTc intervals, and no ST elevations. You do note, however, deep S-waves in leads V2 and V3 and tall R-waves in leads V5 and V6 with associated downsloping ST segments and T-wave inversions consistent with left ventricular hypertrophy (LVH) with a “strain pattern” that you surmise is due to long-standing hypertension (see Fig. 41.1).
A 57-Year-Old Male With Exertional Chest Pain
In the outpatient setting, what are the most likely causes of chest pain?
What features of the patient’s presentation are consistent with chest pain of cardiac origin?
What medications should you prescribe and what tests should you order at this visit?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


