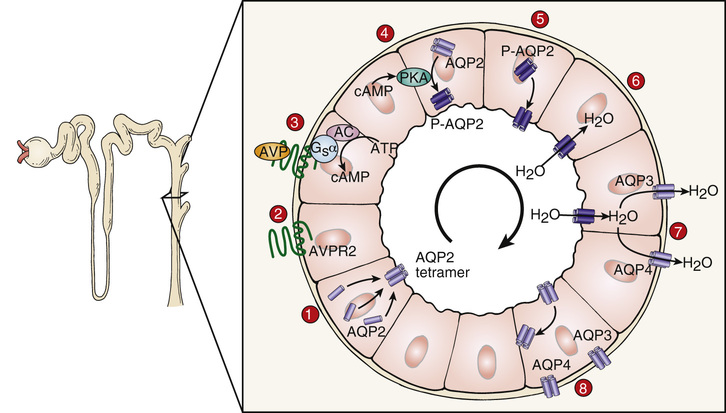
Mark Riley, Patricia Lorenzo, John D. Carmichael It is important to ask about the nature of nocturia when evaluating a patient with a urinary complaint. Under normal circumstances, the kidneys produce less urine during the night, allowing people to sleep through the night without having to urinate. Waking multiple times with the urge to urinate can be pathologic. When a patient presents with polyuria, nocturia, and polydipsia, you should think about the possibility of a hormonal etiology. It is also important to elucidate from the patient what and how much he or she drinks before bed. Because this patient wakes several times during the night to urinate without drinking excess fluids before bed, an endocrine disorder is likely. In a patient with polyuria, a urinalysis can be done to assess urine concentration and check for the presence of abnormal substances or microbes. Because the other chief complaint is polydipsia, electrolyte and serum solute status are important to know as well. These can be obtained with a basic metabolic panel. A glucose and hemoglobin A1C (HbA1C) should also be ordered to evaluate for diabetes mellitus. A urine osmolality less than 200 mOsm/kg in conjunction with polyuria often indicates the presence of diabetes insipidus (DI). DI is a condition in which the kidneys excrete large volumes of dilute urine. Patients with untreated DI produce greater than 3 L/day but can exceed 18 L/day. This excess water loss is attributed to a problem with the normal function of vasopressin, a hormone secreted from the posterior pituitary that facilitates the reabsorption of water in the distal tubules of the kidney. There are several forms of DI: central DI, nephrogenic DI, and primary polydipsia (also called psychogenic DI). Central DI is caused by a dysfunction in the synthesis, transport, or release of vasopressin from the hypothalamus or posterior pituitary. Nephrogenic DI is the result of resistance to the action of vasopressin by the kidneys. Primary polydipsia is the result of chronic excess fluid intake that impairs the release of vasopressin. The normal actions of vasopressin on the nephron act to conserve free water loss in the urine (Fig. 30.1). The treatment for each form of DI is different, so it is important to differentiate which form is present in this patient with further testing before proceeding with treatment. Because the patient shows no signs or symptoms of infection, a urinary tract infection would be low on the differential despite the presence of polyuria. Other conditions that can cause polyuria and polydipsia are diabetes mellitus, kidney failure, hypercalcemia, and medications such as diuretics or lithium.
A 20-Year-Old Female With Polyuria and Polydipsia
Why should you ask about nocturia?
What tests would you order initially?
What is your differential diagnosis at this point?
30 A 20-Year-Old Female With Polyuria and Polydipsia
Case 30