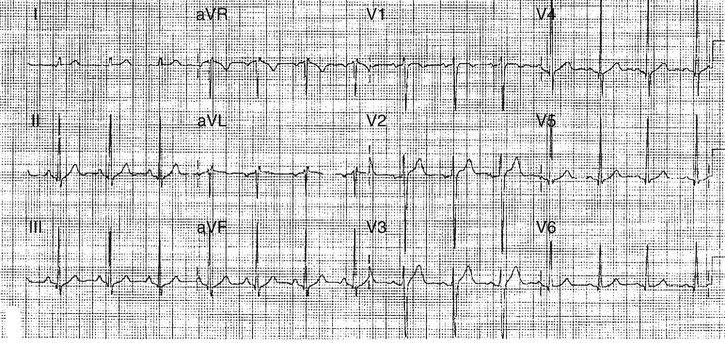
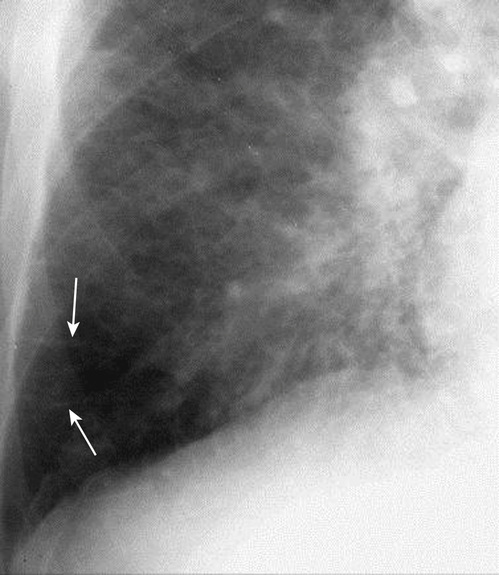
Nida Hamiduzzaman, Seth Politano Differential diagnosis for dyspnea at rest can be caused by heart disease, renal disease, lung disease, or hematologic abnormalities. One must consider acute ischemia or heart disease as a cause of such. Fluid retention from chronic kidney disease, interstitial lung disease, chronic obstructive pulmonary disease, anemia, or bone marrow suppression due to malignancy or chronic infection should be considered as well. On physical exam, the patient’s temperature is 37 °C (98.6 °F), blood pressure is 102/80 mm Hg, pulse rate is 98/min, and oxygen saturation is 88% on room air. Jugular venous distention is present; the lung exam reveals bilateral crackles in lower lobes; the cardiac exam reveals a regular rhythm and an S3 heart sound; and lower extremity edema is present with bilateral pitting to the knees. Laboratory testing reveals a hemoglobin of 11.0 g/dL, creatinine of 1.3 mg/dL, sodium of 133 mEq/L, and troponin of 0.1 ng/mL. The patient’s electrocardiogram (ECG) is shown in Figure 28.1. His chest radiograph is shown in Figure 28.2 You should order a B-type natriuretic peptide (BNP). Serum levels of BNP and N-terminal-pro B-type natriuretic peptide (NTproBNP) increases in response to an increase in ventricular volume and pressure overload. NTproBNP has a longer half-life in the serum than BNP. The plasma half-life of BNP is estimated to be about 20 minutes. Both BNP and NTproBNP are used to help distinguish acute dyspnea caused by heart failure from other non-heart failure causes. Most patients with heart failure have values above 400 pg/mL. Risk factors for heart failure in this case include hypertension, diabetes, dyslipidemia, and history of smoking cigarettes. Other risk factors for heart failure are use of cardiotoxic substances, such as alcohol and cocaine, thyroid disorders, tachycardia, valvular disease, and coronary artery disease (CAD). In obese patients, sleep apnea should be ruled out as it can cause hypertension, which can lead to heart failure. Treatment for risk factors reduces the risk for heart failure.
A 62-Year-Old Male With Dyspnea at Rest and Lower Extremity Edema
What is the differential diagnosis for dyspnea at rest?
What additional laboratory test would you order at this point?
What is the role of BNP?
What are risk factors for heart failure in this patient?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


