CASE 15
A 32-year-old Hispanic woman presented with a cough for several weeks and a 15-lb weight loss. She also had night sweats and subjective fevers and felt fatigued. Despite erythromycin treatment for suspected pneumonia given by her family physician, her fever and cough progressively got worse. She complained about coughing blood-tinged sputum.
LABORATORY STUDIES

Diagnostic Work-Up
Table 15-1 lists the likely causes of illness (differential diagnosis). Any patient with an exposure history (i.e., emigration from an endemic country), with apical infiltrates, and who does not respond to antibacterial agents for community-acquired pneumonia should, however, have appropriate studies to rule out tuberculosis. The investigational approach may include
TABLE 15-1 Differential Diagnosis and Rationale for Inclusion (consideration)
Rationale: The chronic symptoms of fever, cough, night sweats, and weight loss should prompt the suspicion of tuberculosis (TB) in any patient particularly one with upper lobe disease. TB is also much more common in immigrants from developing countries than in those born in the United States. Chronic pneumonia due to endemic fungi (e.g., H. capsulatum) can be indistinguishable from TB and should also be considered, particularly in patients from the appropriate geographic region of the United States. Nocardia and Actinomyces may also cause chronic pneumonia. Aspiration pneumonia is usually seen in patients with poor dentition and altered mental status, such as dementia or chronic alcoholism. The remaining agents are less common causes of chronic pneumonia.
MICROBIOLOGIC PROPERTIES
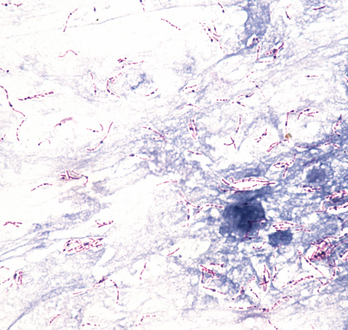
Mycobacteria are acid-fast bacteria (reactive to auramine O fluorescence and Kinyoun acid-fast stains; Fig. 15-2). The cell wall contains 60% lipid in the form of long-chain fatty acids called mycolic acids. M. tuberculosis is the major medically important mycobacterial agent (Table 15-2). M. tuberculosis grows slowly (doubling in 18 hours) on selective (e.g., Lowenstein-Jensen) agar media. Virulent strains grow in parallel and serpentine pattern due to the presence of cord factor (6,6′ trehalose-dimycolate), a virulence factor. The surface macromolecules of M. tuberculosis (e.g., purified protein derivative [PPD, glycolipids]), including species-specific mycosides, are highly antigenic. Phenolic glycolipids (e.g., lipoarabinomannan [LAM]) contribute to enhanced virulence. Mycobacteria are resistant to acid and alkali and are resistant to dehydration.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


