LABOR AND DELIVERY
Objectives
• State the complication related to intravenous fluid administration in the high-risk mother.
• Recognize the different types of fluid administration used in cases of high-risk labor.
Drug calculations for labor and delivery are the same as those used in critical care. Determinations of the concentration of the solution, infusion rates, and titration factors are the primary calculation skills used. Accurate calculations are essential, as is the monitoring of intravenous (IV) fluid intake for medications and anesthetic procedures. Impaired renal filtration in patients with preeclampsia and the antidiuretic effect of tocolytic drugs make the monitoring of fluid intake vital. Accurate measurement of IV fluid intake along with pulmonary assessment can decrease the risk of fluid overload and the sequelae of acute pulmonary edema in women at high risk for complications.
Physicians’ orders and hospital protocols give specific guidelines for administering IV drugs. Carefully labeling all IV fluids, IV medications, and IV lines is essential in preventing drug errors. The nurse is responsible for managing the IV drug therapy, monitoring the patient’s fluid balance, and assessing the patient’s response to drug therapy.
FACTORS INFLUENCING INTRAVENOUS FLUID AND DRUG MANAGEMENT
The most important concept in labor and delivery is that the drugs given to the mother also affect the unborn baby. Therefore the responses of both the mother and the unborn baby must be closely monitored. Vital signs and laboratory results, such as platelet counts, liver function studies, renal function, magnesium levels, reflexes, and contraction patterns, are the main indicators of the mother’s status. For the fetus, the fetal heart pattern is the primary guide.
TITRATION OF MEDICATIONS WITH MAINTENANCE INTRAVENOUS FLUIDS
Women in labor receive IV fluids to prevent dehydration when oral intake is contraindicated. IV drugs are given to stimulate labor, treat preeclampsia, or inhibit preterm labor. Normally, 500 to 1000 mL of IV fluids may be given to initially hydrate the mother, especially in preterm labor or before administration of regional anesthesia. Any IV medications that are given by titration are a part of the hourly IV rate. The patient has a primary IV line and a secondary IV line for medications. All IV medications should be delivered by a volumetric pump, which ensures that the specified volume and correct dosage are delivered.
Titration of drugs is frequently done for women with preeclampsia and women experiencing preterm labor. The most common use of titration is for the induction or augmentation of labor. In the following example, an oxytocic drug is given, and the primary IV rate is adjusted with the secondary IV drug line to achieve a therapeutic effect and maintain adequate maternal hydration. Note that the drug is ordered to be given by concentration and that the infusion rates for volume per minute and hour must be determined.
Administration by Concentration
EXAMPLES
Note: 1 Unit = 1000 milliunits
For the secondary IV set, the following calculations must be made:
2. Infusion rates: volume per minute and volume per hour.
3. Titration factor in concentration per minute (milliunits/min).
For the primary IV set, the following calculations must be made:
Secondary IV (see Chapter 8 for formulas)

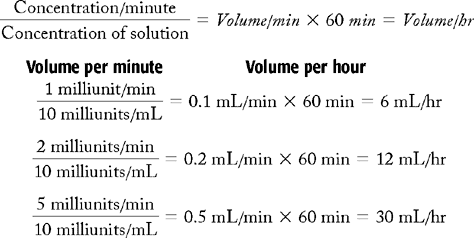
3. Titration factor (see Chapter 12): To increase the concentration by increments of 1 milliunit/min, the hourly rate on the pump must be increased by 6 mL/hr. The titration factor for this problem is 6 mL/hr. To increase the concentration to a higher rate, multiply the rate of increase times 6 mL/hr. (Example: To increase infusion to 5 milliunits/min, multiply 5 by 6 mL = 30 mL/hr.)
For the secondary IV line, the concentration of the solution is 10 milliunits/mL of oxytocin, with the infusion rate of 6 mL/hr to be increased in increments of 1 to 2 milliunits every 15 to 30 minutes until contractions are 2 to 3 minutes apart.
Primary IV
The secondary IV rate will start at 6 mL/hr; therefore the primary rate will be 94 mL/hr. (A balance is needed to achieve 100 mL/hr.)
For every increase in rate from the secondary line, a corresponding decrease must be made with the primary IV line. If the rate of the secondary line exceeds the ordered hourly rate, the primary IV line may be shut off completely. The concentration of the solution may be changed by the physician if the mother is receiving too much fluid.
Administration by Volume
In the previous example, the oxytocin was ordered to be infused by concentration (milliunits/min), which is the recommended method for patient safety. Sometimes in clinical practice, the infusion rate may be ordered by volume (mL/hr).
EXAMPLES
Mix 30 units of oxytocin in 500 mL NSS. Start at 1 mL/hr and increase by 1 to 2 mL every 15-30 min until uterine contractions are 2 to 3 minutes apart. Notify physician before exceeding 40 milliunits/min.
To determine the concentration per hour of infusion, multiply concentration of the solution by volume/hr = concentration/hr:

To determine the concentration of the infusion per minute, divide:
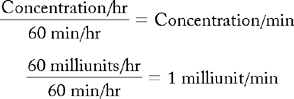
Therefore an oxytocin solution with a concentration of 60 milliunits/mL infused at 1 mL/hr will administer 1 milliunit of the drug per minute.
INTRAVENOUS LOADING DOSE
Some situations require IV medications to be infused over a short period to obtain a serum level for a therapeutic effect. This type of IV drug administration is called a loading dose.
In the following example, a patient with preeclampsia receives a loading dose of magnesium sulfate, followed by a maintenance dose of magnesium sulfate via the secondary IV line. A primary IV line is also maintained after the loading dose is given. At the end of this example, the total IV intake is determined for an 8-hour period.
EXAMPLES
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


