Plastic and Reconstructive Surgery
LEARNING OBJECTIVES
After studying this chapter the reader will be able to:
• Indicate the primary reasons for plastic and reconstructive surgery
• Describe the surgical anatomy and physiology associated with the integumentary system
• Recognize the special considerations for burns
• Identify grafts, implants, and prostheses relevant to plastic and reconstructive surgery
• Summarize the surgical technologist considerations related to plastic and reconstructive surgery
• Discuss the procedural steps involved in plastic and reconstructive surgery
Overview
Derived from the Greek word plastikos, which means to mold or give form, plastic surgery is a medical specialty that restores or gives shape to the body. There are two different subspecialties of plastic surgery. Cosmetic surgery restores or reshapes normal structures of the body, to improve appearance and self-esteem. Reconstructive surgery treats abnormal structures of the body caused by birth defects, developmental problems, disease, tumors, infection, or injury to restore function and correct disfigurement or scarring (American Society of Plastic Surgeons [ASPS], 2009a.) As a surgical specialty, plastic surgery owes much of its heritage to knowledge gained from the wars of the twentieth century (History box).
Despite the economic downturn, 12.1 million cosmetic surgical procedures were performed [by surgeons certified by the American Society of Plastic Surgeons (ASPS)] in 2008, an increase of 3%; the majority were minimally invasive procedures. Females constituted 91% of all patients undergoing cosmetic procedures. Hispanic, Asian, and African American patients showed an increase in cosmetic procedures; the number of Caucasians undergoing cosmetic procedures decreased by 2%. Office-based cosmetic procedures increased by 13%, with a total of $10.3 billion dollars spent on the cosmetic procedures in the United States (Ambulatory Surgery Considerations). The 4.9 million reconstructive procedures also showed a 3% increase, although breast reductions decreased by 16% (ASPS Stats, 2009).
Surgical Anatomy
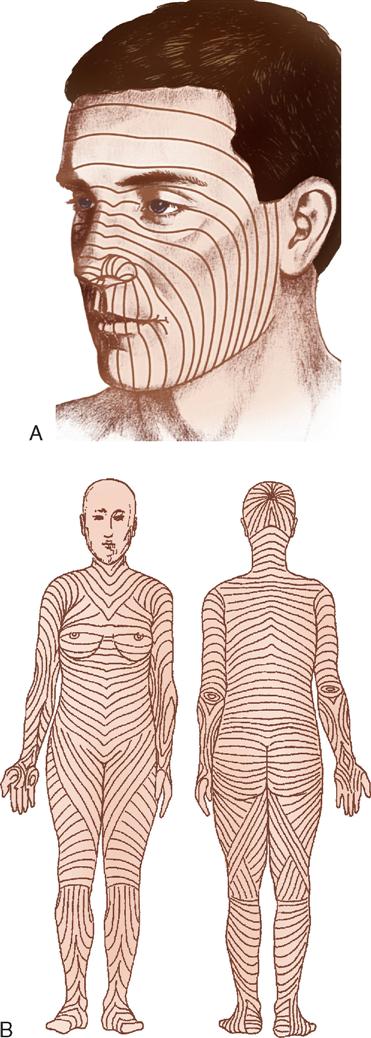
Plastic and reconstructive surgery is not limited to a single anatomic or biologic system. It is based on thorough understanding of the anatomy and biology of tissue. Operative techniques are complex and staged to achieve the expected results. The surgery also involves removing, reducing, enlarging, and recontouring, as well as camouflaging scars into existing skin lines (Figure 13-1). The tissues of the body can be transferred to use as various types of flaps. Free flaps are the transfer of tissue along with its vascular pedicle. When nerve is anastomosed with these flaps, they are called neurovascular free flaps. Flaps are used to cover defects or create new structures such as breasts, digits, or facial structures. Body parts can also be transplanted. By improving the patient’s deformity, the patient’s self-esteem will improve and the patient will feel more comfortable in public and social activities. The body changes as we age. The patient’s concern with aesthetics, the variety of acquired defects, the diversity of operative techniques, and the psychologic responses of patients offer unique learning experiences and challenges for perioperative patient care.
Surgical Technologist Considerations
Preparation of the OR Suite.
Assemble all necessary medical and surgical supplies, equipment, suture material, positioning aids, implantable devices, and medications. Ensure that lights and video equipment are in working order, that emergency supplies are present, and that compressed gases are adequate. Depending on the procedure to be performed, the OR bed may need to be configured differently from the standard room setup. Plastic and reconstructive surgeons frequently use preoperative photographs of the patient when attempting to restore or modify appearance. These photographs help the surgeon maintain perspective since features may change because of surgical positioning. Preoperative and postoperative photos, in order to be accurate, should be taken with the same lighting, angle, and distance (Hagan, 2008).
Equipment and Special Mechanical Devices.
Essential equipment for any OR includes a fully functional bed that may be positioned for any number of special needs and also has accessory attachments, such as headrests and aids for extremity positioning. The room must also have well-positioned and numerous electrical outlets, good overhead lighting, suction equipment, mounted x-ray view boxes, and computer terminals for those facilities using electronic medical records. Step stools, tables, chairs, hand tables, tourniquets, microscopes, and intravenous (IV) poles should be in appropriate supply and accessible. Surgeons often provide their own digital cameras although facilities may have them available for use.
INSTRUMENTATION.
Basic instrument trays are available for the plastic surgery OR. A “local” tray may include Bishop Harmon and adson tissue forceps (with and without teeth); straight and curved iris, Stevens, and Metzenbaum scissors; fine mosquito forceps; and skin hooks. Minor and major trays for plastic surgery may contain a range of tissue forceps, scissors, hemostats, and retractors. With the addition of instruments for specific surgeries, these trays usually suffice for all plastic surgery operations. Adequate instrumentation should be available to avoid flash sterilization (Risk Reduction strategies).
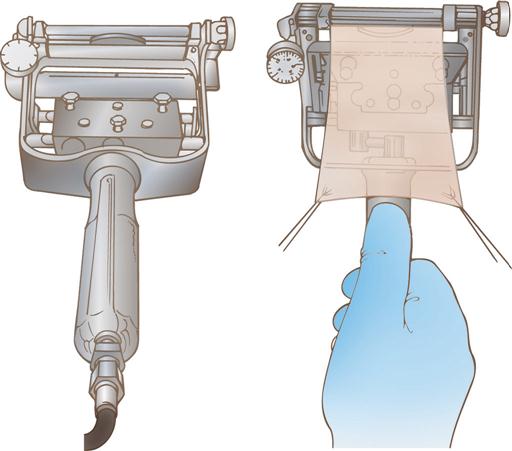
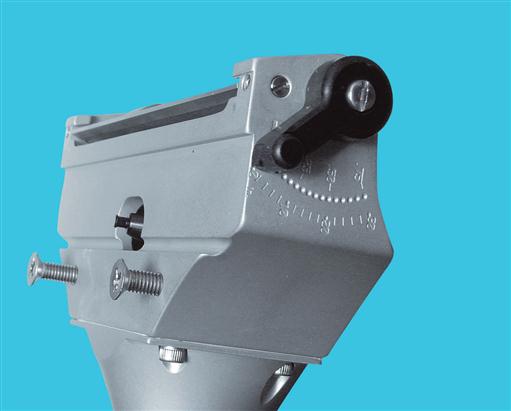
DERMATOMES.
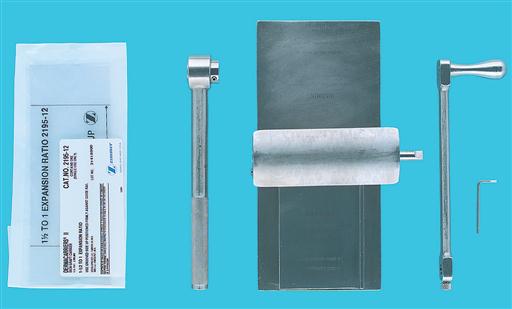
Dermatomes are used for removing split-thickness skin grafts (STSGS) from donor sites; they are of three basic types: knife, drum, and motor-driven (Figures 13-2 through 13-5). Sterile mineral oil and a tongue blade should be available when stsgs are being obtained.


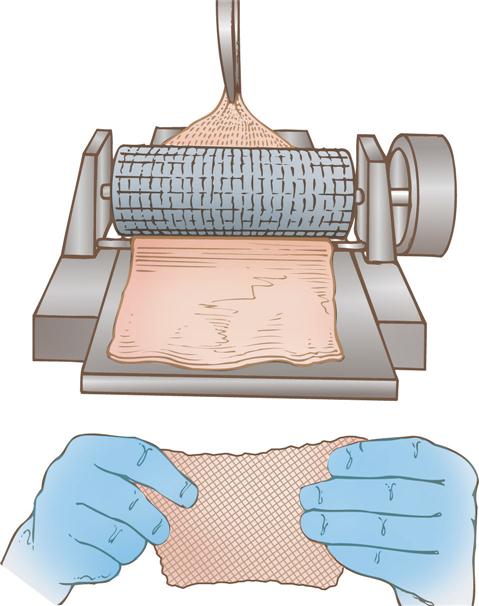
SKIN MESHERS.
Several types of skin meshers are available. Each is designed to produce multiple uniform slits in a skin graft, approximately 0.05 inch apart. These multiple apertures in the graft can then expand, permitting the skin graft to stretch and cover a larger area. Meshing also facilitates drainage through the graft, preventing fluid accumulation under a graft. The graft is placed on the carrier and passed through the mesher (Figures 13-6 and 13-7). The manufacturer supplies sterile carriers for meshers. They are usually available in several sizes, which determine the expansion ratio of the skin graft.
PNEUMATIC-POWERED INSTRUMENTS.
Pneumatic-powered instruments use an inert, nonflammable, and explosion-free compressed gas as their power source. The motor may be activated by a foot pedal or hand control. The various attachments should be sterilized as recommended by the manufacturer to prolong instrument life and ensure effective sterilization. The following attachments may be used in plastic surgery:
A pneumatic tourniquet with an inflatable cuff is used in most hand surgery procedures as well as in other upper and lower extremity surgical interventions. The tourniquet is described in Chapter 10.
ELECTROSURGICAL UNIT.
The electrosurgical unit (ESU) is employed and safety precautions should be followed. Monopolar ESU will require the use of a grounding pad (return electrode/dispersive electrode). Specialized tips will be used with the ESU pencil including needle point and guarded along with the standard tip. The use of specialized tips allows the use of higher coagulation settings to obtain hemostasis with little or no effect on adjacent tissue or structures. Inspect ESU tip and cord on handpiece for damage before use, be sure tip is securely seated into the place handpiece in nonconductive holster when not in use, keep tip free of eschar or tissue build-up. Methods to do so include moistened sponge, instrument wipe, and abrasive electrode cleaner, but not a scalpel blade.
BIPOLAR COAGULATION UNIT.
Bipolar electrosurgery is the use of electrical current in which the circuit is completed by means of two parallel poles located close to one another. One pole is positive; the other is negative. The flow of current is restricted between these two poles, which are usually the tines of the bipolar forceps. Because the poles are so close, low voltages are used to achieve the tissue effect. Because electrical current does not flow through the patient, a return electrode (dispersive pad) is not necessary. This makes bipolar electrosurgery very safe and permits precise electrocoagulation.
LASERS.
A variety of lasers are employed for plastic surgical procedures. The perioperative team must ensure that the laser safety accessories specific to the type of laser being used are available. Types of lasers and their common uses are presented in Box 13-3, pp. 637–639.
BOX 13-3
Common uses for lasers in plastic surgery include exfoliation, treatment of vascular malformations, removal of hair and tattoos, and tightening of collagen fibers in aging skin. A variety of lasers are available; selection of the appropriate laser is dependent on the patient’s diagnosis because the effect of the laser on the skin tissue is dependent on its wavelength. The types of lasers and their common uses are described below.
| Laser | Use |
| CO2 | Desiccation of benign lesions of skin, skin resurfacing, cutting tissue |
| Excimer | Eye surgery, psoriasis |
| Argon | Hemangiomas, telangiectasias |
| Nd:YAG | Benign pigmented lesions and red tattoos |
| Candela dye | Tattoos, pigmented benign lesions, hemangiomas |
| Helium-neon | Biostimulation, wound healing alleviation, acupuncture |
| Diode | Hair removal, tattoo removal |
| Ruby | Nevi removal, dark tattoos |
| Erbium: YAG | Rhytides |
| Q-Switch | Benign pigmented lesions and dark tattoos |

Modified from Choi JE et al: Treatment of Becker’s nevi with a long-pulse alexandrite laser, Dermatol Surg, April 27 [Epub ahead of print], 2009; Kono T et al: Long-pulsed neodymium:yttrium-aluminum-garnet laser treatment for hypertrophic port-wine stains on the lips, J Cosmet Laser Ther 11(1):11-13, 2009; Krupashankar DS: Standard guidelines of care: CO2 laser for removal of benign skin lesions and resurfacing, IADVL Dermatosurgery Task Force, Indian J Dermatol Venereol Leprol 74(suppl):S61-S67, 2008; Mendonca DA et al: Venous malformations of the limbs: the Birmingham experience, comparisons and classification in children, J Plast Reconstr Aesthet Surg, Dec 27 [Epub ahead of print], 2008; Onesti MG: Surgical and laser treatment of Sturge-Weber syndrome, Aesthet Plast Surg, Mar 19 [Epub ahead of print], 2009.
FIBEROPTIC INSTRUMENTS.
Examples of fiberoptic instrument attachments used in plastic surgery are a headlight for rhinoplasties, augmentation mammoplasties, and other procedures; a mammary retractor for augmentation mammoplasties; a rhytidectomy retractor; abdominoplasty retractors; and endoscopic face and forehead fiberoptic instrumentation.
LOUPES.
Loupes (Figure 13-8) are magnifying lenses used by many plastic surgeons for microvascular surgery and nerve repairs and for numerous other instances in which cosmetic results are improved by the magnification effect. The nurse should inquire about the use of loupes before the surgeon dons a headlight because adjustments will need to be made to the headlight alignment if the loupes are required in midprocedure. Adjusting or removing the headlight in midprocedure has the potential to contaminate the sterile field.

MICROSCOPE.
The microscope is frequently used in nerve repairs and microsurgical anastomoses; the nerves or vessels to be repaired, such as in hand surgery, and the suture used to do so (sometimes 9-0, 10-0, or even 11-0 size) can be finer than human hair and thus requires magnification. While each microscope has different features, an important matter to avoid confusion is whether the surgeon control overrides the assistant view, or if each can separately adjust the field of view.
WOOD’S LAMP.
The wood’s lamp is an ultraviolet lamp used in a darkened room to determine the viability of skin flaps. After IV injection of fluorescein, the blood vessels appear bright purple (the skin appears yellow). Sodium fluorescein is excreted in the urine, and patients should be informed of this.
SPECIAL SUPPLIES.
Surgeon-specific and procedure-specific special supplies are frequently added to instrument setups for plastic and reconstructive procedures. these commonly include the following: sterile marking pen or methylene blue; ruler; local anesthetic of choice for injection, with syringes and needles; and ESU, with active electrode (pencil) and tip of choice, with tip cleaner.
Sutures.
Sutures range from permanent to absorbable and include monofilament and multifilament materials. The surgical technologist should be a good steward of costly resources and should verify the type and number of sutures needed before opening suture packages, as well as needle preference, to prevent waste. Many plastic surgical procedures have multiple techniques, each of which necessitates very specific suture choices.
Dressings.
Dressings are an essential part of the operative procedure in plastic surgery and may contribute to the ultimate outcome of the surgical intervention. Dressings are usually applied while the patient is still anesthetized. In general, the dressing should accomplish the following five goals:
1. Immobilize the surgical part.
2. Apply even pressure over the wound.
4. Provide comfort for the patient.
Pressure dressings may be used to eliminate dead space, to prevent seroma and hematoma formation, and to prevent third spacing associated with liposuction and reconstructive procedures involving transfer of large muscle or tissue flaps. In some cases pressure can be achieved by the use of catheters or drains placed within the operative site and connected to closed-wound suction devices, such as a Hemovac or Jackson-Pratt. In smaller wounds a butterfly cannula may be inserted into the operative site, with the needle end placed into a red-top tube, such as a blood collection tube, that has a vacuum (evacuated tube).
Common general dressings and supplies available in sterile form and various sizes:
♦ Nonadherent gauze (e.g., Betadine gauze, Adaptic, Nu Gauze, Xeroform, Biobrane, Scarlet Red)
♦ Petrolatum gauze, ½ inch (or other packing material, such as Merocel sponge for nasal packing)
♦ Telfa
♦ Gauze dressing sponges, 4 × 4 inches, 2 × 2 inches
♦ Kling, Kerlix fluff, and Kerlix gauze rolls (2, 4, and 6 inches wide)
♦ Abdominal pads (most commonly used are 5 × 8 inches)
♦ Webril
♦ Tape (paper; silk; and foam; skin tapes, flesh-colored and regular [1/8, 1/4, 1/2, and 1 inch wide])
♦ Benzoin spray or swab or Mastoplast
♦ Coban
♦ Casting supplies and splints (as required for postoperative immobilization)
♦ Abdominal binders and other postoperative garments
♦ Slings
In some instances, such as a free flap, transparent dressings are used so that the flap can be monitored and observed for vascular flow. Compression garments and support devices are also frequently used by plastic surgeons. Proper fit is essential to minimize vascular compromise. Compression garments are typically applied over a light dressing. A proper garment is selected based on its characteristics (e.g., fabric, stretch, softness, antimicrobial properties) and proper sizing according to measurement instructions. Educating patients of the needs and benefits of compression garment use as well as providing hints for their proper application (avoid ripping with long nails, instructions on how to don the garment) promotes comfort and compliance (Gladfelter, 2007).
Implant Materials.
The range of materials available for implantation and augmentation in the specialty of plastic and reconstructive surgery has benefited from ongoing research. The perioperative team is responsible for complying with tracking regulations for implantable materials and devices (Patient Safety).
Biologic materials (autogenous grafts) are preferred when available. Autologous human tissue successfully utilized includes fat, solid dermis, and collagen. Human cadavers are used as a source for acellular collagen (AlloDerm) (Figure 13-9). This product is available in various sizes of sheeting and must be rehydrated in several steps. AlloDerm integrates with the body’s tissue and helps to prevent rejection over the long term.
Implant failure may be directly linked to bacterial contamination; therefore meticulous aseptic technique with minimal handling is essential when using implants of any sort. Most alloplastic implants are presterilized from the manufacturer.
Anesthesia.
A variety of anesthesia techniques are employed with plastic surgery procedures. Local, regional, tumescent, conscious sedation, deep sedation, and general anesthesia may be used, depending on the type of procedure, the patient’s anesthetic history, the American Society of Anesthesiologists (ASA) physical status classification, and the surgeon’s preference.
Preoperative Skin Preparation.
Most surgical interventions require that the operative site and adjacent areas be cleansed before surgery. The physician may prescribe that the patient carry out this treatment before surgery. Special attention is given to the fingernails for patients undergoing hand surgery; to hair for surgery of the head, face, or neck; and to oral hygiene for surgery in or near the mouth. Shaving is avoided and clippers, not a razor, are used if needed, because shaving creates an access for the entry of bacteria into the operative site (Health Stream, 2007). The eyebrows and eyelashes, in particular, are left intact to preserve facial appearance and expression. The surgical site is marked before surgery by the surgeon to designate the correct site and to define landmark areas. Either a povidone-iodine solution, an iodine-alcohol mixture, chlorhexidine gluconate (CHG), or another broad-spectrum agent may be selected for the antimicrobial skin prep. The use of CHG should be avoided around the ears and eyes. It is important to place shields on the eyes if prepping the periorbital site or performing an extensive head and neck prep, place plugs in the ear canals, and prevent pooling of the prep agent. When prepping for a skin graft procedure, separate skin prep setups are needed for the graft and donor sites.
Positioning and Draping.
The OR bed must be positioned so that the remaining space in the room can comfortably accommodate anesthetic equipment, members of the surgical team, instrument tables, and any adjunct equipment (hand table, drills, microscope, laser) to be used. The patient is carefully positioned on the OR bed so that all operative sites may be appropriately exposed and the airway easily observed and accessed.
SURGICAL TECHNOLOGY PREFERENCE CARD
Plastic and reconstructive surgery patients will range from infant to adult and include corrections for birth defects, trauma, burns, cancers, and cosmetic reasons.
Planning with the perioperative team is essential in plastic and reconstructive surgery with a wide variety of surgical procedures and patient populations. Specialty supplies, instruments, and prostheses will be used, frequently requiring strict sterile technique and efficient room layout. Allowing additional time preoperatively to organize the room and check the availability of supplies and prostheses provide for efficient communication between the circulator and scrub during the procedure. Additional setups for some procedures may be needed, so additional furniture and equipment should be organized to ensure sterility and no mixing of instruments.
Room Prep: Basic operating room furniture in place, thermoregulatory devices, padding, positioning supplies, ESU, and in some cases laser or a microscope
Prep Solution: In room and may require more than one site prepped
Catheter: In the room and correct size for patient
PROCEDURE CHECKLIST
Instruments
Specialty Suture
Hemostatic Agents
Specialty Supplies
Additional Supplies: both sterile and nonsterile
Medications and Irrigation Solutions
Drains and Dressings
Specimen Care
Before opening for the procedure, the surgical technologist should:
♦ Damp dust lights, furniture, and surfaces
♦ Verify functionality of equipment
♦ Place items to be opened in their appropriate places
♦ Ensure all prosthesis sizes are on hand if one is to be used
When opening sterile supplies:
Correct draping procedures depend on the location of the operative site or sites. Disposable drapes are often used because of their barrier qualities, ease of handling and storage, and versatility in adapting to a variety of plastic surgery procedures. Two of the most frequently used draping techniques in plastic surgery are the head drape and the hand drape. Both of these draping techniques have the goal of providing maximum mobility of the operative part. The head drape includes a fluid-resistant drape that encircles the head and the addition of a drape to cover the remainder of the body. The following techniques represent methods of obtaining maximum accessibility and sterile coverage for facial surgery:
Surgical Interventions
Reconstructive Plastic Surgery
Reconstructive plastic surgery seeks to restore or improve function after trauma, disease, infection, congenital anomalies, or acquired defects while trying to approximate an aesthetic appearance.
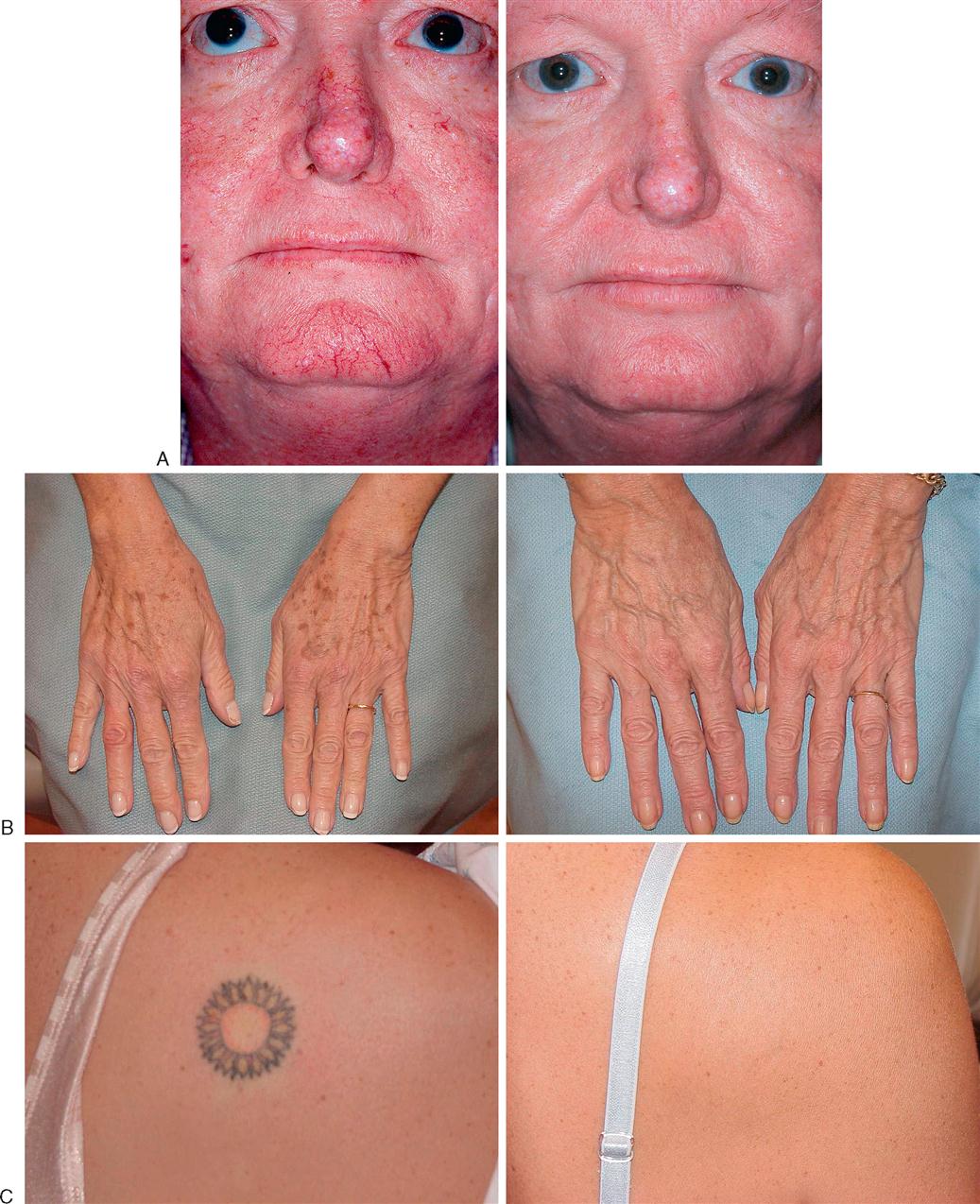
REMOVAL OF SKIN CANCERS
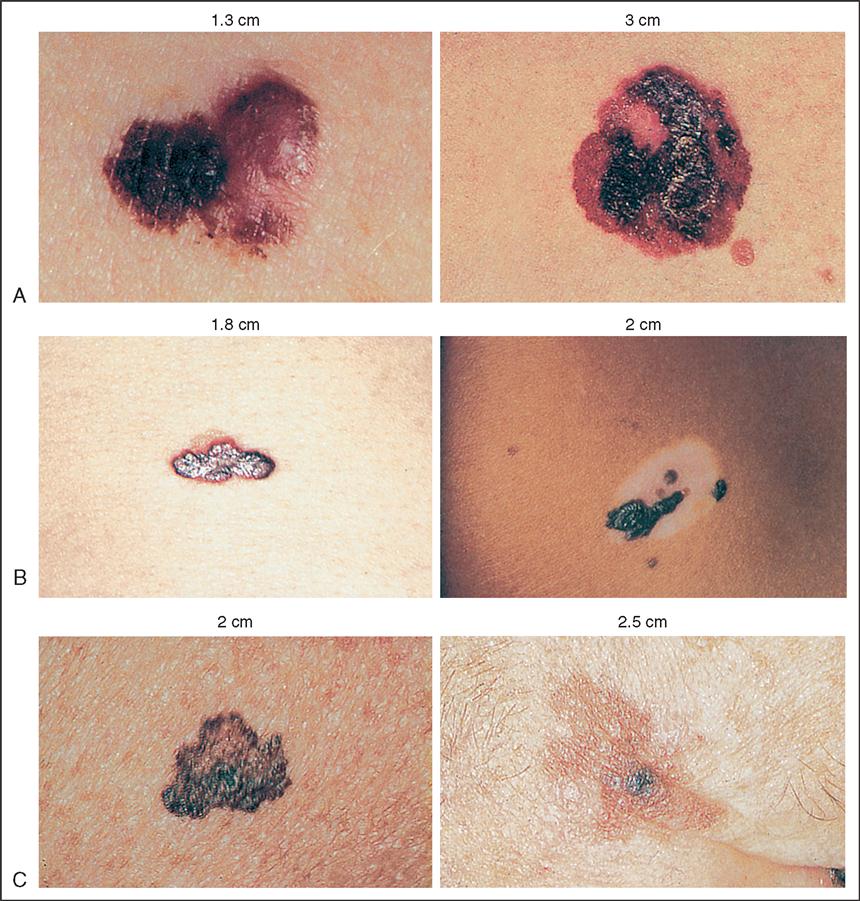
The estimated number of new skin cancer cases diagnosed in 2009 is 1 million (National Cancer Institute [NCI], 2009). The three most common skin cancers are basal cell, squamous cell, and melanoma (Gutierrez and Peterson, 2007). Basal cells account for approximately 70% of all skin cancers (Figure 13-10, A). If basal cell cancer is left untreated, it will grow locally, but rarely metastasizes (Box 13-1). Treated early, it may be cured by simple excision and closure (with pathologic diagnosis to ensure disease-free margins). Squamous cell skin cancers are considered more aggressive (Figure 13-10, B). Surgical treatment is the same as that for basal cell carcinomas. Melanoma accounts for the smallest percentage of skin cancers (5%), but it is treated much more aggressively because of its high mortality rate, comprising 75% of skin cancer deaths (Sladden et al, 2009) (Figure 13-10, C). Excision of melanoma may involve sentinel node mapping and excision. Early diagnosis of melanoma is imperative to successful treatment (Evidence for Practice). A Cochrane Database Systematic Review is underway (Sladden et al, 2009) since various international organizations varied in their recommendations regarding optimal excision margins. Excision margins that are too narrow may result in higher local recurrence rates and/or mortality; wider excisions may increase hospital length of stay and require costlier procedures such as skin grafting and anesthesia.

Procedural Considerations
Consideration must be given to the type of skin cancer to be excised and the anticipated closure technique. Simple excision and closure with adjacent tissue will be the simplest technique, requiring a local plastic tray accompanied by skin markers and the electrosurgical unit (ESU), and usually involving use of a local anesthetic with epinephrine. A simple excision may be performed with the patient administered a local or general anesthetic or after induction of sedation. If additional procedures will be performed (e.g., reconstruction with skin graft, flap, or sentinel node mapping), refer to those sections for additional procedural considerations.
Operative Procedure—Simple Excision
Mohs’ Surgery
Mohs’ surgery is a specialized excision used to treat basal and squamous cell skin cancers. The procedure involves excising the lesion layer by layer and examining each layer under the microscope until all the abnormal tissue is removed.
Procedural Considerations.
Mohs’ surgery is usually completed on an ambulatory basis with the patient administered a local anesthetic. The procedure can be very time-consuming to accomplish, but it typically results in the preservation of the surrounding healthy tissue. Because the procedure is lengthy, patient preparation and comfort are essential to facilitate cooperation during the procedure. A minor plastic surgery set is required, along with fine (5-0 or 6-0) suture material.
Operative Procedure.
Current procedures involve removal of all visible portions of the skin cancer lesion. A horizontal layer of tissue is removed and divided into sections that are color-coded with dyes. A map of the surgical site is then drawn. Frozen sections are immediately prepared and examined microscopically for any remaining tumor. If tumor is found, the location or locations are noted on the map and another layer of tissue is resected. The procedure is repeated as many times as necessary to completely remove the tumor.
BURN SURGERY
A majority of burns result from exposure to high temperatures, which injures the skin. Flame, scalding, or direct contact with a hot object may cause thermal skin injury. Similar destruction of skin can result from contact with chemicals such as acid or alkali or contact with an electrical current. The latter, however, often involves extensive destruction of the underlying tissue and physiologic systems in addition to the skin. A 2007 fact sheet on burn statistics includes the following information: approximately 500,000 burn injuries receive medical treatment yearly; 40,000 patients are hospitalized in the United States for burn injuries, with 25,000 of those admitted to the 125 hospitals with specialized burn centers (American Burn Association [ABA], 2007).
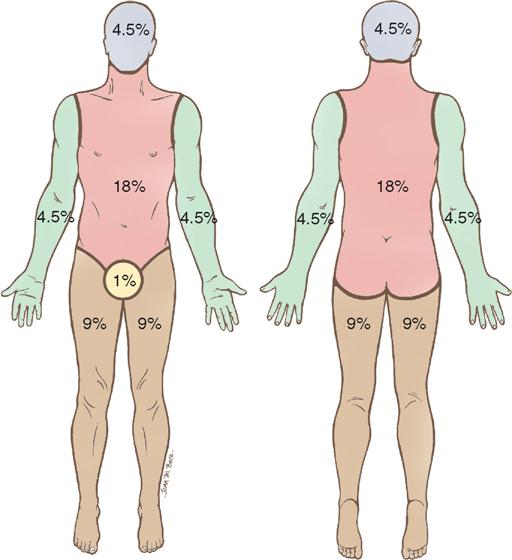
Intact skin provides protection against the environment for all underlying tissues and organs. It aids in heat regulation, prevents water loss, and is the major barrier against bacterial invasion. The tissue injury resulting from a burn disrupts this normal protective function, resulting in local and systemic effects (Box 13-2). Burn patients are therefore some of the most acutely ill patients brought to the OR. The greater the degree of injury to the skin, expressed in percentage of total body surface area (BSA) and depth of burn, the more severe the injury. One method of measuring BSA in adults is by use of the rule of nines (Song et al, 2007) (Figure 13-11).
Partial-thickness (first- and second-degree) burns heal by regeneration of skin from dermal elements that remain intact. First-degree burns involve the epidermis, which appears pink or red; sunburn is usually a first-degree burn. Second-degree burns, also called partial-thickness burns, involve the epidermis and some of the dermis. Full-thickness (third-degree) burns (Figure 13-12) involve the epidermis, the entire dermis, and the subcutaneous tissues; they require skin grafting to heal because no dermal elements remain intact. Both partial- and full-thickness burns may require debridement of necrotic tissue (eschar) before healing can occur by skin regeneration or grafting. An allograft may be used to cover the burned area during the initial healing process. However, the allograft must be carefully tested for immunodeficiency diseases. A xenograft (e.g., pig skin) may also be used for covering the burned area.

Procedural Considerations
The essentials of skin grafting are discussed under Skin and Tissue Grafting. This section therefore deals only with the procedure for debridement of burn wounds.
A basic plastic instrument set is required, plus a knife dermatome, an ESU, topical thrombin solution, a pneumatic tourniquet for isolated extremity burns, and a topical antimicrobial agent of choice.
Because patients who have sustained burns are vulnerable to hypothermia from the loss of body surface area (BSA), the temperature and humidity in the OR are increased and exposure is limited only to the areas related to the planned surgical event. Anesthesia is often induced while the patient is on the burn unit bed; transfer to the OR bed is done carefully and gently, with attention to maintaining the airway. Most burn patients arrive in the OR with dressings covering their wounds. The dressings are removed after the patient has been anesthetized to minimize pain and loss of body heat through the open burn wounds. Throughout the procedure, the temperature in the OR is constantly monitored to prevent hypothermia. The OR team caring for burn patients coordinates activities to prevent any delays in obtaining required equipment or supplies. A variety of topical agents are used to dress wounds.
Melanoma Awareness, Prevention, and Detection
It is estimated that more than 68,720 men and women will be diagnosed with melanoma in 2009, according to the American Cancer Society. In the most recent time period, rapid increases have occurred among young white women (3.8% annual increase since 1995 in those aged 15 to 34 years) and older white men (8.8% annual increase since 2003 in those 65 and older). Although the exact cause of developing a melanoma is not known, certain risk factors have been identified:
♦ Ultraviolet (UV) radiation: sunlight, tanning beds
♦ Moles: more than 50 = greater risk
♦ Fair skin: fair skin, freckling, red or blond hair
♦ Family history: 10% have a relative with melanoma
♦ Immune system compromise: taking antirejection medications after organ transplantation surgery
♦ Age: increased risk in older adults
♦ Previous melanoma: increased risk for having another melanoma
PREVENTION
Limit UV radiation exposure:
KNOW YOUR A-B-C-Ds
A: Asymmetry—one half of the lesion looks different from the other side.
B: Border irregularity—instead of a smooth edge, the border is ragged or irregular.
C: Color—the color is usually irregular as well; may have a number of different hues and colors.
D: Diameter—lesions larger than 6 mm have a greater chance of being a melanoma.
Modified from American Cancer Society (ACS): Cancer facts and figures 2009, Atlanta, 2009, The Society.
Operative Procedure
1. The surgeon excises all nonviable tissue down to underlying muscle fascia.
3. Hemostasis is obtained with the ESU or use of topical thrombin solution.
4. Dressings saturated with the topical antimicrobial agent of choice are applied.
Although skin grafting may be done at the time of wound debridement, it is usually performed several days later, particularly in burns that are extensive.
EXCISIONAL DEBRIDEMENT
Excisional debridement is the act of removing dead or devitalized tissue to promote healing. Plastic surgeons use debridement in conjunction with treatment of injuries, trauma, and infection.
TREATMENT OF PRESSURE ULCERS
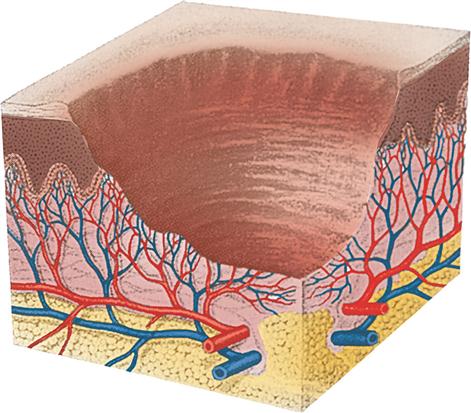
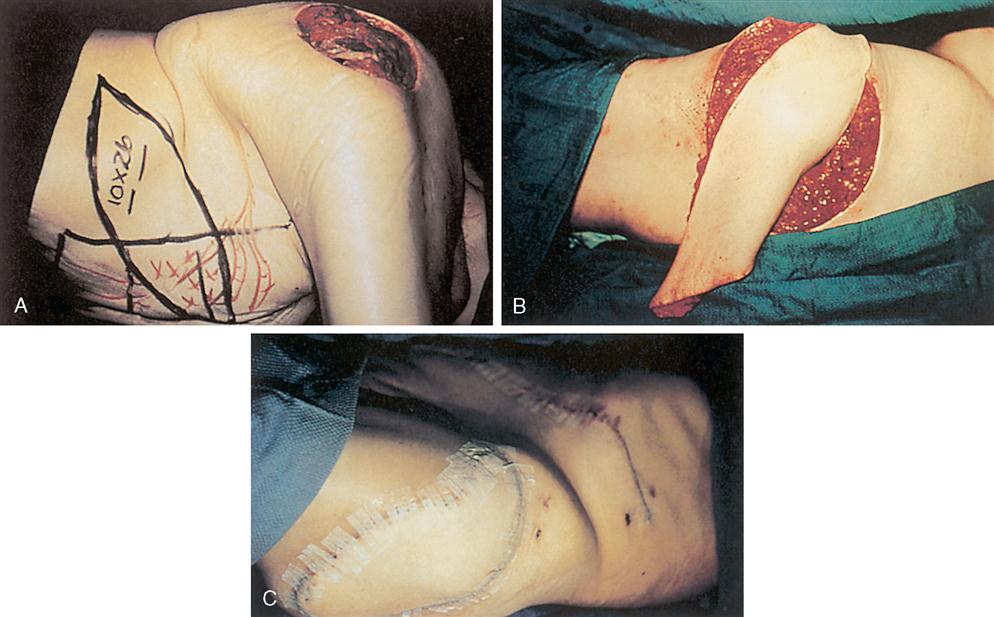
Pressure ulcers result from prolonged compression of soft tissues overlying bony prominences (Figure 13-13). However, whether excessive pressure is sufficient to create an ulcer depends on the intensity and duration of the pressure as well as on tissue tolerance. Factors that contribute to pressure ulcer development are immobility, sensory and motor deficits, reduced circulation, anemia, edema, infection, moisture, shearing force, friction, and nutritional debilitation (Cuzzell and Workman, 2010). The most common sites of pressure ulcers are the sacrum, the ischium, the trochanter, the malleolus, and the heel; these are called decubitus ulcers. These ulcers are different from chronic ulcers such as vascular, diabetic, and neurogenic ulcers. Surgical interventions for pressure ulcers are usually based on ulcer staging (also referred to as grading). In stage I the ulcer involves the epidermis and has soft tissue swelling that is irregular and ill-defined; heat and erythema at the ulcer site are characteristic. A stage II ulcer involves the epidermis and dermis but not the subcutaneous fat. Stage III ulcers show full-thickness skin loss with injury to underlying tissue layers and may contain necrotic material. Thorough excisional debridement is performed, and IV antibiotic therapy is instituted. Although debrided stage III ulcers often heal on their own, surgical excision and closure may be done to prevent a lengthy spontaneous closure, which may result in a weak, unstable scar with resultant recurrence. Stage IV ulcers are the deepest, requiring more radical excisional debridement. Adequate soft tissue cover may be obtained by either split-thickness or full-thickness skin grafting or tissue flaps (Figure 13-14). Tissue expansion may be used when there is not enough tissue adjacent to the ulcer site to provide flap coverage.
The use of a CO2 laser minimizes blood loss and possibly reduces infection rates in the presence of gross contamination. Although many techniques and flaps are surgical options, basic principles apply to all pressure ulcer closure procedures. The following procedure is for an adjacent flap.
Procedural Considerations
A basic plastic instrument set is required, as well as assorted sizes of osteotomes (straight and curved), a mallet, the Gigli saw and handle, assorted curettes, a Key periosteal elevator, a duckbill rongeur, bone wax, the dermatome of choice, the ESU, a sterile marking pen, and a closed-wound drainage system. The patient is positioned and draped so that the pressure ulcer, adjacent flap donor site, and skin graft donor site are well exposed.
Operative Procedure
Topical Medications Used in Burn Therapy



