Morphine Sulfate

CLASSIFICATION
Analgesic, opioid agonist
ACTIONS
Interacts at a specific receptor-binding site. Agonist activity at the receptor site can result in analgesia, euphoria, depression, hallucinations, miosis, and sedation. Alters pain at the spinal cord and higher levels in the central nervous system (CNS) (Schedule II on Controlled Substances Act).
USES
• Relieves mild-to-severe pain.
• Decreases anxiety, therefore decreases myocardial oxygen demands with pain from a myocardial infarction.
CONTRAINDICATIONS
• Intracranial pressure and suspected head injuries; may mask the development of increased intracranial pressure (IICP)
• Hepatic and renal dysfunction
PRECAUTIONS
• Seizures, asthma, and severe respiratory depression
SIDE EFFECTS
• †Respiratory depression†
• Urinary retention, **confusion**
• **Constipation,** nausea and vomiting
• **Orthostatic hypotension**
• Tolerance and physical dependency with long-term use
• Toxicity: coma, respiratory depression, and pinpoint pupils
NURSING IMPLICATIONS
1. Perform strict documentation and inventory assessment of narcotic.
2. *Assess pain and vital signs (especially respirations) before and after the dose; do not administer if respirations are below 12 breaths per minute.*
3. Infants and older adults are very sensitive to depression of respirations.
4. *Naloxone (Narcan) reverses the effect of morphine.*
5. Medication of choice for patient-controlled analgesic (PCA).
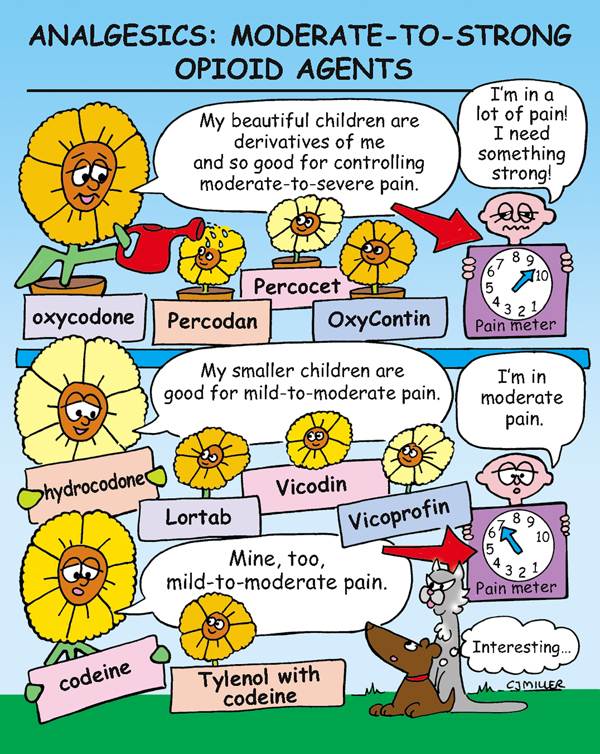
Analgesics: Moderate-to-Strong Opioid Agents

ACTIONS
Bind with receptors in the brain and spinal cord that are associated with pain. Moderate opioid analgesics are similar to morphine; however, pain control is less effective, and the potential for respiratory depression is less.
OPIOID ANALGESICS
• Percodan—combined with aspirin.
• Percocet—combined with acetaminophen.
• Combunox—combined with ibuprofen.
• OxyContin—controlled release, dosing is usually every 12 hours with another analgesic for breakthrough pain.
• Lortab—combined with acetaminophen.
• Vicodin—combined with acetaminophen.
• Vicoprofen—combined with ibuprofen.
• May also be combined with antihistamines and nasal decongestants for cough suppression.
codeine—PO, IV, IM, SQ Schedule II
• Tylenol with codeine (PO) for mild pain relief.
• Frequently combined with various agents for suppression of cough.
NURSING IMPLICATIONS
1. *Assessment is critical to effective pain control. Carefully assess patient’s level of pain and administer analgesic as ordered.*
2. Follow institution procedure for Controlled Substance Act.
3. Reassess patient 1 hour after administering medication.
4. *Administer medication before pain returns; fixed schedule of dosing may be more efficient than “as needed” dosing.*
5. *The majority of hospitalized patients do not receive adequate medication to relieve pain; therefore concern for addiction while hospitalized is usually not warranted.*

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


