CHAPTER 11. CENTRAL VENOUS CATHETER INSERTION
NICE guidelines on ultrasound guidance90
Indications91
Contraindications91
Equipment91
Practical procedure91
Placement of femoral lines100
Complications101
Post-procedure investigations and care101
Measuring central venous pressure using a manometer101
Equipment101
Practical procedure102
Post-procedure investigations103
Suggested reading104
Stephen Hales (1677–1761) performed the first recorded central venous catheterization in 1733 when he inserted a glass tube into the jugular vein of a horse to measure central venous pressure. In 1953 Seldinger described a percutaneous method for central venous access, and subsequently central venous cannulation became a widespread medical technique.
INTRODUCTION
Modern central venous catheters have several lumen, which allow for:
Central venous catheters can be placed in the internal jugular, subclavian or femoral veins using the Seldinger technique. This chapter will discuss internal jugular and femoral approaches.
NICE GUIDELINES ON ULTRASOUND GUIDANCE
• 2D imaging ultrasound guidance should be the preferred method when inserting a central venous catheter in adults and children in elective situations.
• 2D imaging ultrasound guidance should be considered in most clinical situations where central venous catheter insertion is necessary, either elective or emergency.
• When using the ultrasound, ensure that the orientation of the probe correlates with the anatomical position. The probe head should have a marker on one side that corresponds to a marker on the screen, enabling the user to identify correct orientation of the probe (and hence correct orientation of the vessels you are visualizing!).
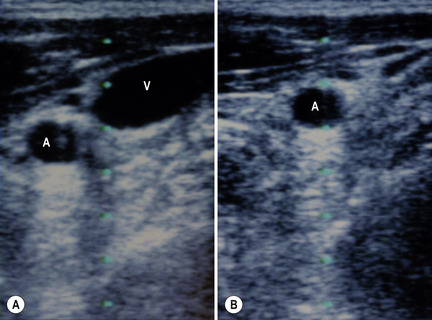
• Having found the internal jugular or femoral vessels, check for the vein by compressing the region with the probe. The vein collapses with the application of pressure whereas the thicker-walled artery remains patent and pulsates (Fig. 11.1 A and B).
INDICATIONS
• Measurement of central venous pressure.
• Secure intravenous access in patients requiring several lumens for i.v. infusions.
• Pre-operatively for major operations, e.g. aortic aneurysm repair, coronary artery bypass grafts; these are usually inserted by anaesthetists.
CONTRAINDICATIONS
• Coagulopathy (relative contraindication).
• Local sepsis over puncture site.
• Lack of consent.
EQUIPMENT
• Dressing pack.
• Sterile gown, gloves and drapes.
• Chlorhexidine cleaning solution.
• Lidocaine.
• 2 × 10 mL syringes.
• 1 × 5 mL syringe.
• Orange needle.
• 2 × green needles.
• Sterile gauze.
• 100 mL sterile bag normal saline.
• Central line pack (includes central line, introducer needle, guidewire and dilator).
• 3-way taps (the quantity corresponding to the number of lumens on the central line).
• Scalpel.
• Suture.
• Clear sterile dressing.
• If available – portable ultrasound probe, sterile cover and probe jelly.
PRACTICAL PROCEDURE
POSITIONING FOR INTERNAL JUGULAR LINE PLACEMENT
• Lay the patient flat on the bed and elevate the bed to your level for your own comfort.
• Tilt the bed with the head down (the Trendelenburg position). This reduces the risk of air embolism whilst also helping to distend the neck veins.
 Tip Box
Tip BoxIf the patient is more dyspnoeic in the head-down position, minimize the time spent in this position by performing the skin preparation and infiltration of local anaesthesia with the patient sitting up.
• Turn the patient’s head approximately 30 degrees from the midline away from the side of line insertion.
 Tip Box
Tip BoxIf the patient is inadvertently flexing their neck, place a 0.5- or 1-L bag of normal saline between the shoulder blades; this allows for more neck extension.
 Tip Box
Tip BoxPlace the patient on telemetry in order to observe for potential arrhythmias during insertion. These occur if the guidewire or line is inserted too far and makes contact with the tricuspid valve, in which case pull back the guidewire.
PREPARATION
• Wash hands, wear the sterile gown and gloves and lay out sterile environment and dressing pack.
• Check and assemble the equipment – attach three-way taps to all lumens of the central line other than the port through which the guidewire will pass. Flush the ports with normal saline to ensure patency (simply pierce the sterile bag of normal saline with a green needle attached to a 10 mL syringe and withdraw saline as required). Once flushed, turn the 3-way taps off to the patient.
 Tip Box
Tip BoxAfter flushing the lines, keep the saline flush syringe on top of the normal saline so as not to confuse it with the lidocaine syringe.
• Clean the area – clean outwards in a spiral motion from the centre to the periphery.
• Place a sterile drape over the patient with a central window over the area of line insertion.
• Palpate the carotid artery and ultrasound the area in order to obtain a guide of the anatomy and landmarks for insertion (Fig. 11.2).
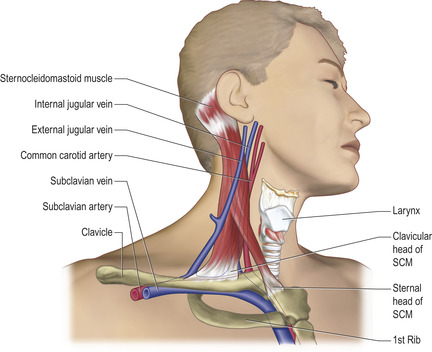 |
Fig. 11.2 Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|