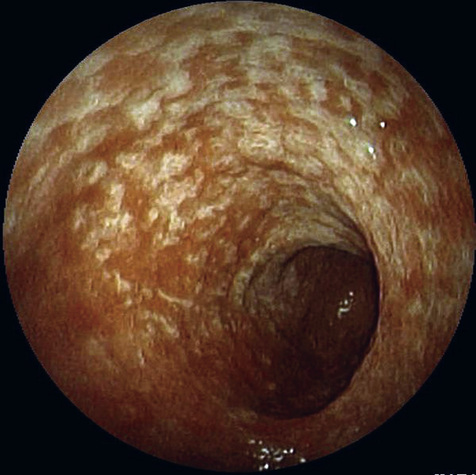
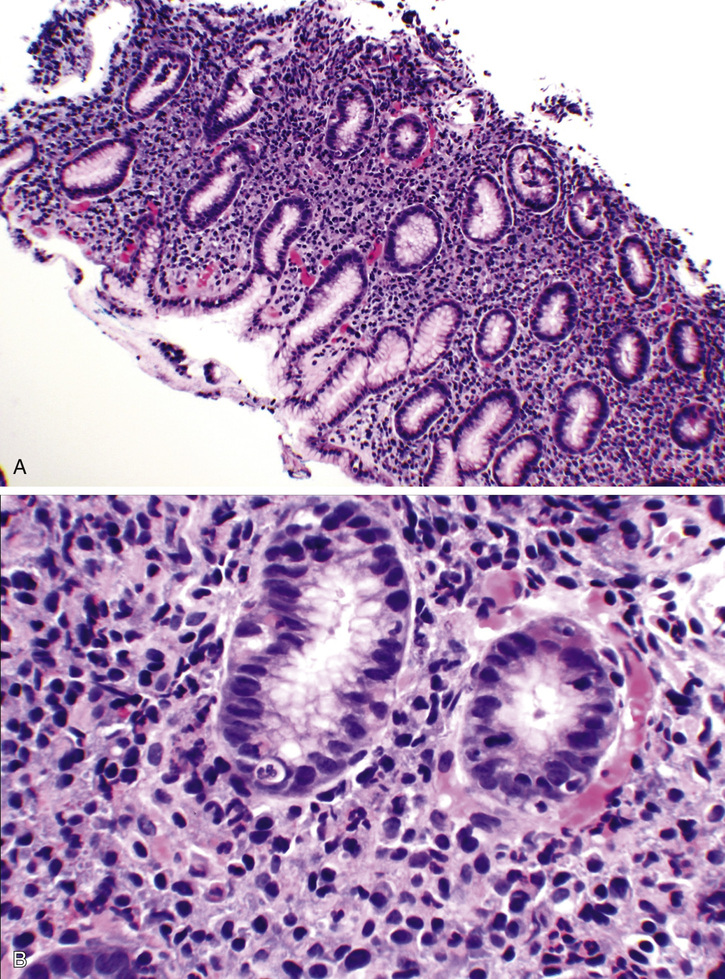
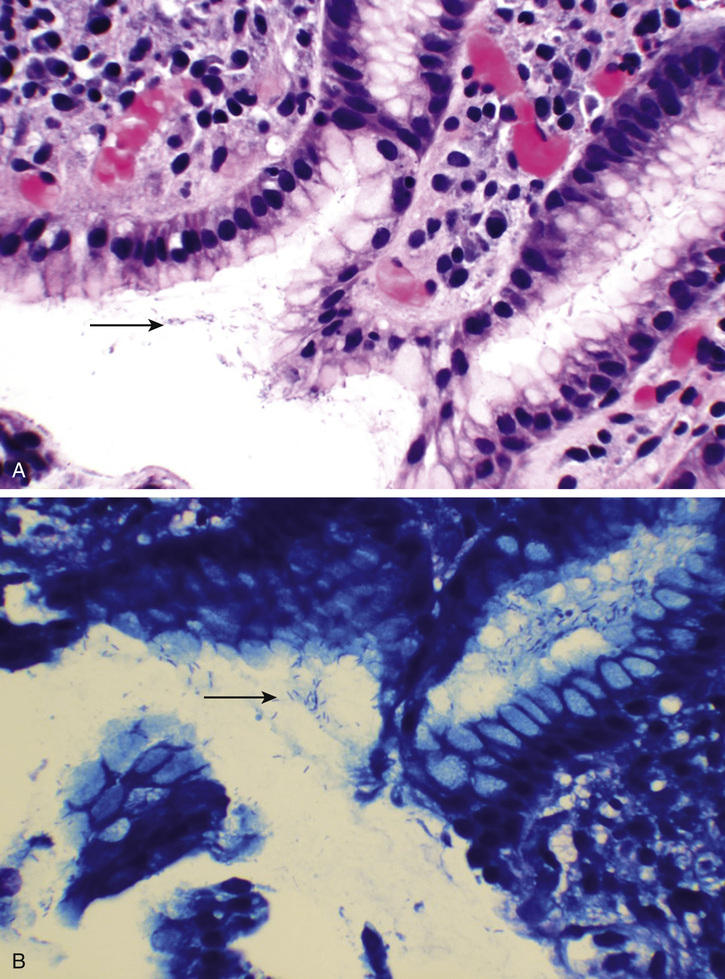
Monisha Bhanote, Daniel Martinez The clinical vignette is a classic setup for peptic ulcer disease/gastritis or gastroesophageal reflux disease (GERD) given the description of the pain and following risk factors: older age, chronic NSAID use, alcohol/tobacco use, and stress. Another reasonable common pathology to consider is biliary colic given the description of a recurrent dull epigastric pain. Because of her age, an astute clinician would also consider other pathologies such as a gastric malignancy (adenocarcinoma or mucosa-associated lymphoid tissue [MALT] lymphoma) or a pancreatic head mass. However, these are less likely given that she has no red flags such as a concerning family history, weight loss, jaundice, or lymphadenopathy. Given her classic symptoms and lack of red flags, empiric treatment with a proton pump inhibitor (PPI) such as omeprazole is appropriate at this time. Endoscopy is commonly performed first when the patient is over 45 years old and has weight loss, anemia, or heme-positive stools. Upper endoscopy can help find causes of unexplained symptoms such as heartburn, nausea, vomiting, and problems swallowing. It can also help with abnormal lab results such anemia and nutritional deficiencies. She arrives at her gastroenterologist and an EGD is scheduled. She tolerates the procedure well; after the procedure, her gastroenterologist explains that visually her esophagus and duodenum are unremarkable. However, her stomach did show areas of erythema (Fig. 10.1), which suggests gastritis, and biopsies were taken to confirm. He advises her to return for a follow-up and explanation of the biopsy results. Findings commonly see in abnormal endoscopy are erosions, antral nodularity, thickened gastric folds, and visible submucosal vessels. Although these findings are not specific for a particular type of gastritis, the presence of a mosaic pattern in the corpus of the stomach may suggest a Helicobacter-type gastritis. The patient returns to her gastroenterologist for follow-up, and he informs her that the biopsies were positive for Helicobacter pylori infection. Specifically, the pathology revealed an active gastritis with expansion of the lamina propria with inflammatory cells such as lymphocytes, plasma cells, and neutrophils as well as numerous small curved organisms identified in the intercellular spaces of the foveolar cells. They are seen in the hematoxylin and eosin (H&E) stain but are better appreciated with a Giemsa stain (Figs. 10.2 and 10.3). The patient was confirmed to have a H. pylori gastritis with the biopsy. H. pylori is a curved, gram-negative rod bacterium that produces urease. It is an infection that is normally acquired in childhood. Colonization with this bacterium is not a disease in itself; however, it is associated with a number of disorders in the upper gastrointestinal tract. H. pylori infection can be diagnosed with serology, stool antigen testing, urea breath test, and biopsy. Serology can be positive up to 18 months after eradication. The most reliable method, however, is with biopsy and histologic exam combined with either a rapid urease test or microbial culture. Stool antigen testing is a common way of evaluating for infection in patients with typical symptoms and no red flags. If the patient were young, testing for stool antigen would have been the next step in management after she failed the trial of omeprazole. Step 2/3 Clinical Pearl
A 62-Year-Old Female With Epigastric Pain and Nausea
What pathologies should you be thinking about in this patient? How should you proceed?
When is an EGD indicated?
What are common visual findings of gastritis on EGD?
How is Helicobacter pylori infection diagnosed?
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


10 A 62-Year-Old Female With Epigastric Pain and Nausea
Case 10
{kind=link}
