CHAPTER 1 From Neurons to Acupoints: Basic Neuroanatomy of Acupoints
INTRODUCTION
The efficiency of acupuncture therapy is based on the selection of effective acupoints. There are 361 classic meridian acupoints, and more than 2000 new extrameridian acupoints have been recorded in the Chinese literature on acupuncture. Anatomic examination of the 361 classic meridian acupoints shows that most acupoints are associated with certain anatomic structures of the peripheral nervous system (PNS). Researchers have indicated that 309 acupoints lie on or near the nerves and that 286 acupoints are situated next to major blood vessels, which are surrounded by small nerve bundles.1
Modern neuromuscular medicine named some of these points trigger points, motor points, and dermopoints. Dr. Ronald Melzack2 found that more than 70% of the classic meridian acupoints correspond to commonly used trigger points. Whatever terms are used, all these points are characterized by the ability to become painful or tender or to create other physical discomforts as a result of sensitized nerves. It is extremely important to understand that although more than 70% of the classic acupoints share the same characteristics as trigger points, acupoints and trigger points are not the same.
In their book Muscle Pain, Drs. Siegfried Mense and David G. Simons define trigger points as follows: “(1) A central trigger point is a tender, localized hardening in a skeletal muscle. Clinical characteristics include circumscribed spot tenderness in a nodule that is part of a palpably tense band of muscle fibers, patient recognition of the pain evoked by pressure on the tender spot as being familiar, pain referred in the pattern characteristic of trigger points in that muscle, a local twitch response, painful limitation of the stretch range of motion, and some weakness of that muscle. Diagnostic criteria of active trigger points are circumscribed spot tenderness in a nodule of a palpable taut band and patient recognition of the pain, evoked by pressure on the tender spot, as being familiar. Latent trigger points cause no complaint of clinical pain. (2) Attachment trigger points have tenderness in the region of muscle attachment caused by enthesitis or enthesopathy induced by the persistent tension of the taut band muscle fibers.”3
In laboratory and clinical experiments, acupuncture stops being effective in a region supplied by a sensory nerve when that nerve is blocked by local anesthesia, cut by surgery, numbed by ice (low temperature), or bound by a band.4 These experiments prove that sensory nerves are vital anatomic components of acupoints. Sensory nerves are distributed all over the human body and are absent on only a few structures, such as nails and hair. Thus where there are sensory nerves there will be acupoints.
The Chinese doctors of ancient times noticed that, in addition to meridian acupoints, some nonmeridian acupoints are as effective as classic meridian points. The two types of nonmeridian acupoints are Ashi acupoints and extrameridian acupoints. Ashi acupoints appear unpredictably in relation to individual symptoms. Extrameridian acupoints are not located on any of the 14 meridians but have fixed locations on the body. Gradually more and more extrameridian acupoints were recorded and incorporated into the classic acupuncture system. The recent Chinese acupuncture literature has recorded more than 2500 “new” acupoints.
In the last three decades, an impressive number of modern studies show that acupuncture efficacy does not always depend on the precise location of acupoints as indicated on meridian charts.5 Scientific data suggest that there is no statistical significance between needling either “sham” or “true” acupoints in treating patients with chronic pain.6 Well-known clinician Dr. Felix Mann, after many years of observation, has concluded that acupoints, in the classic understanding, do not exist at all.7
Tender acupoints appear on the bodies of both healthy persons and pain patients alike. Let us look at a healthy person first. Dr. H.C. Dung discovered that tender acupoints appear in a generally consistent and predictable pattern. Dr. Dung provided an anatomic explanation for why acupoints appear in such a predictable pattern (see Chapter 2). This discovery is regarded as “a turning point in acupuncture’s long history.”8
BASIC NEUROANATOMY FOR DEFINING ACUPOINTS
Neuron (Nerve Cell)
A neuron, or nerve cell, is the anatomic and physiologic unit of the nervous system. Neurons vary in size, shape, and complexity (Figure 1-1). All neurons share common structural and functional features. Typically a neuron has one or more processes, called dendrites, radiating from the cell body. The endings of the dendrites are called receptors.
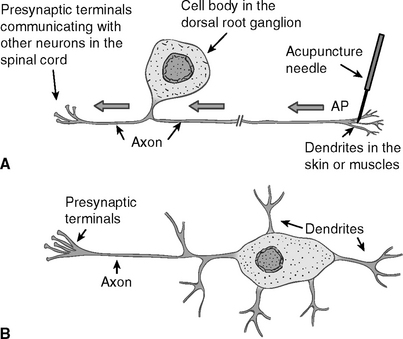
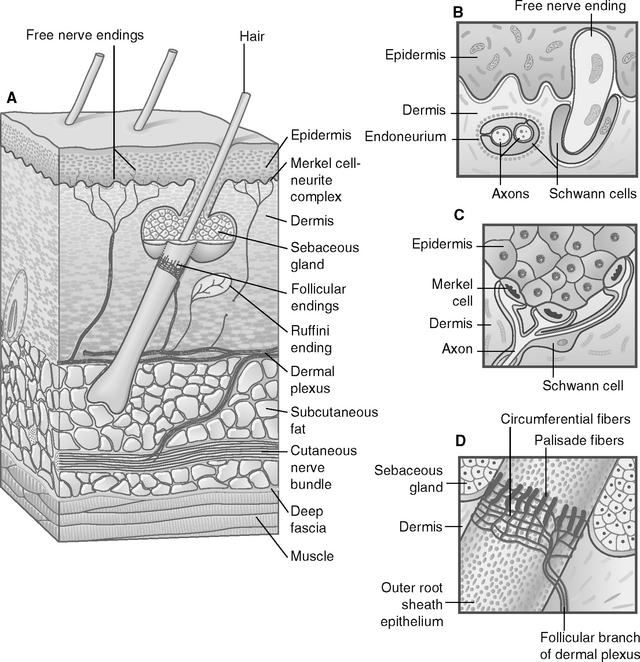
Acupuncture needles directly stimulate and activate the dendrite receptors of the sensory neurons in the skin, muscles, and other soft tissues. Figure 1-2 shows some of the sensory nerve endings (receptors), such as free nerve endings and encapsulated nerve endings.
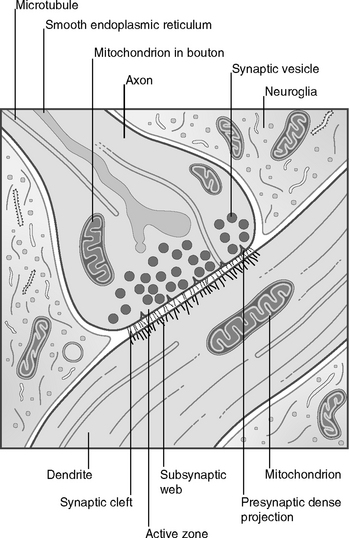
Another single process, called an axon, extends from the cell body (see Figure 1-1). An axon of a sensory neuron sends the impulses from the cell body to the next neuron, or an axon of a motoneuron brings the impulses to the muscles. Stimulation of the receptors by acupuncture needling generates electrical signals, which travel from receptors along the dendrites to the cell body and then to the axon. Stimulation below the threshold will not generate incoming signals to the brain. When stimulation to the receptors is strong enough, it will initiate in the cell body a transient electrical signal called an action potential, which will propagate from the cell body along the axon to the axon terminal. The axon terminal passes the signals to the dendrites or cell body or axon of another neuron through a special structure called a synapse. Thus signals generated by receptors are transmitted from one neuron to another neuron and finally reach the brain (Figure 1-3).
The Central Nervous System
A neuron is a major functional unit in the nervous system. The CNS consists of the brain and the spinal cord. Electrophysiologic9 and neurochemical research shows that both the brain and the spinal cord actively react to acupuncture stimulation. Today, after more than three decades of research, we know more about the involvement of the CNS in acupuncture therapy, but the exact mechanism of this correlation is still unclear. We briefly discuss this mechanism in Chapters 3 and 4.
The Peripheral Nervous System
The PNS consists of the cranial nerves from the brain and the spinal nerves from the spinal cord, a total of 12 pairs of cranial nerves and 33 pairs of spinal nerves. Traditionally Roman numerals are used to designate the cranial nerves. Among them, the trigeminal nerve (V), facial nerve (VII), and spinal accessory nerve (XI) are the most important in acupuncture therapy (Figure 1-4).
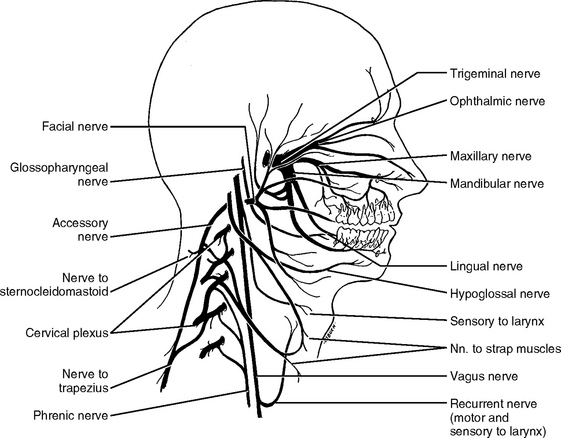
Figure 1-4 The cranial nerves accessible by acupuncture needling in the head and neck: trigeminal nerve (V, three branches: ophthalmic, maxillary, and mandibular), facial nerve (VII), and accessory nerve (XI). Also note that, activated by acupuncture stimulation, the vagus nerve plays a very important role in restoring homeostasis and antiinflammatory immune reaction (see Chapter 4 for further explanation).
(From Jenkins D: Hollinshead’s functional anatomy of the limbs and back, ed 8, Philadelphia, 2002, WB Saunders.)
According to their location in relation to the spinal cord, the 33 pairs of spinal nerves are categorized into five groups: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 3 coccygeal. The coccygeal nerves are less important in acupuncture because of their relatively small size, although severe pain in the coccyx or tailbone may occur and will need to be attended (Figure 1-5).
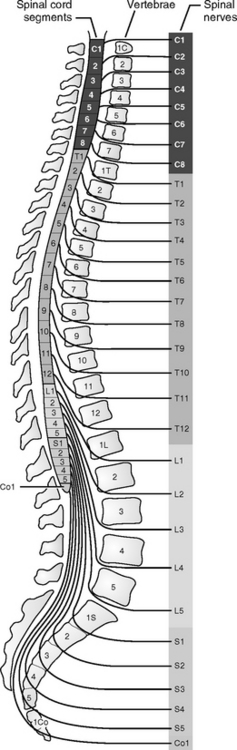
Figure 1-5 The spinal nerves that make up most of the peripheral nerves of the body.
(From Jenkins D: Hollinshead’s functional anatomy of the limbs and back, ed 8, Philadelphia, 2002, WB Saunders.)
The PNS also contains ganglions, which are groups of nerve cells outside the spinal cord. The nerve fibers of the PNS are distributed to all areas of our body except the nails or hair, which is why nails and hair can be cut without pain.
Somatic Nervous System
We classify the nervous system into the CNS and the PNS according to anatomic structure. Functionally we divide the nervous system into two groups: the SNS and the ANS. The SNS is the part of the nervous system that innervates the structures of the body wall: muscles, skin, and mucous membranes. The part of the nervous system that controls visceral organs is referred to as the ANS. From the viewpoint of acupuncture therapy, the SNS is similar to parts of the PNS.
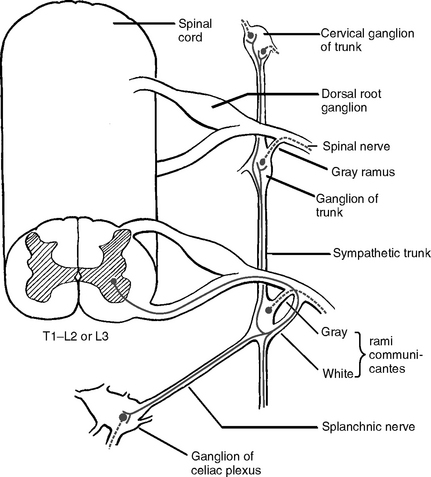
Autonomic (Visceral) Nervous System
Anatomically the efferent components, the outflow pathway of the ANS, are characterized by a two-neuron chain (Figure 1-6). The first neurons, or the primary neurons, are located in the CNS in the brainstem nuclei (groups of neurons in the brain are called nuclei) or in the lateral gray column of the spinal cord.