Splenectomy and Splenorrhaphy
Demetrios Demetriades
Lydia Lam
Introduction
The importance and role of the spleen remained unknown until the 1950s when its hematological and immunological functions were described. Although the surgical management of the spleen in hematological diseases has remained largely unchanged over the last few decades, the management of splenic trauma has undergone numerous significant changes. With better understanding of the role of the spleen, the emphasis of management of splenic trauma switched to spleen-preserving operations and later on to nonoperative management. In more recent years, angiointervention was added to the armamentarium of the surgeon.
The spleen is about 10 cm in length and weighs 75 to 100 g in normal individuals. It is protected posteriorly by the 9th to 12th ribs, but is also exposed to injury when fractures of these ribs occur. It is held in place by the splenogastric, splenocolic, splenophrenic, and splenorenal ligaments (Fig. 1). The splenogastric ligament contains numerous vessels, including five to seven short gastric vessels, which originate from the splenic artery and feed the greater curvature of the stomach. The rest of the ligaments attach the spleen to the diaphragm, to the Gerota’s fascia of the left kidney, and to the splenic flexure of the colon. They contain very few vessels and can be taken down with electro coagulation and sharp dissection. Other attachments often exist between the omentum and the splenic hilum or the superior pole. Careless retraction and tension on these ligaments may cause iatrogenic capsular tears and troublesome bleeding (Fig. 2).
The splenic artery is a branch of the celiac trunk and travels along the superior aspect of the pancreas, leading to the hilum of the spleen where it branches into the upper and lower polar arteries (Fig. 1). These branches travel in a radial direction and dissection in parallel to the vessels make partial splenectomy possible (Fig. 3). The splenic artery may give its branches near the hilum or up to 5 to 10 cm away from it. Appreciation of this anatomical variability may help during splenectomy.
The splenic vein courses more posterior and inferior to the artery and drains into the portal vein after receiving the inferior mesenteric vein and joining with the superior mesenteric vein.
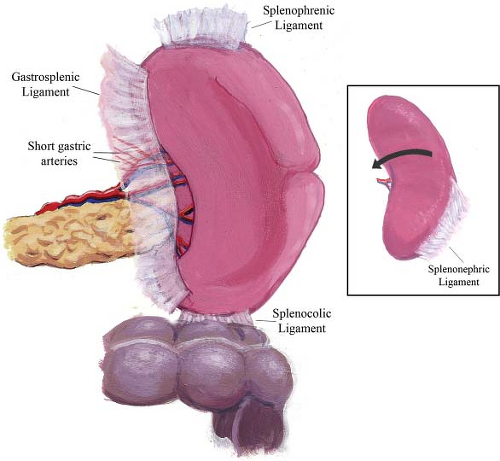 Fig. 1. Splenic ligaments and vessels: The gastrosplenic ligament contains the short gastric vessels and branches of the splenic vessels before they enter the spleen. The splenocolic ligament may contain a few vessels. The splenophrenic and splenorenal ligaments are largely avascular. |
Accessory spleens may be found in many patients, especially those with hematological disorders. They are usually located in the hilum of the spleen, the splenic ligaments, and the greater omentum.
Physiology
The spleen is a key organ for the removal of old or abnormal red cells, platelets, and neutrophils from the circulation. In addition, it plays an important immunological role and is essential in the production of IgM, tuftsin, properdin, and interferon.
Splenectomy for Nontrauma
Nontraumatic indications for splenectomy are typically hematologic conditions, which may affect red cells, white cells, or platelets.
(Table 1) In addition, splenectomy may also be performed for splenomegaly, which causes pain and discomfort to the patient. Because of the significant immunologic role of the spleen, splenectomy should be the last resort, when other therapeutic modalities fail.
(Table 1) In addition, splenectomy may also be performed for splenomegaly, which causes pain and discomfort to the patient. Because of the significant immunologic role of the spleen, splenectomy should be the last resort, when other therapeutic modalities fail.
Table 1 Non-Trauma Diseases that May Require Splenectomy | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
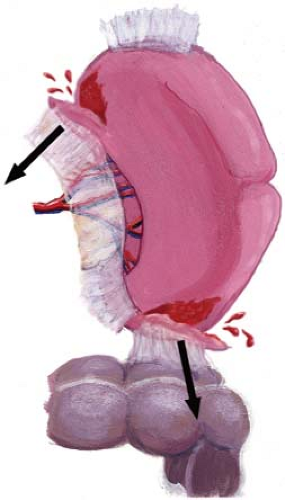 Fig. 2. Excessive retraction of the spleen, stomach, or the colon may cause capsular avulsion and troublesome bleeding. |
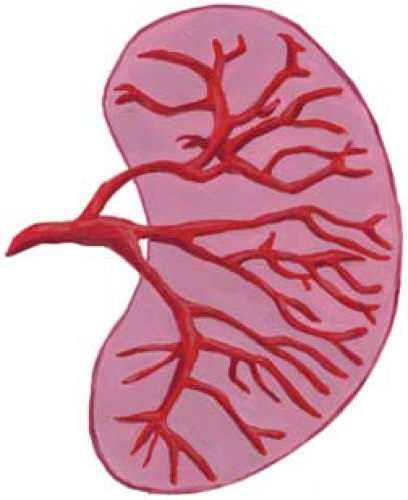 Fig. 3. The intrasplenic branches of the splenic vessels travel in a radial direction. Dissection parallel to the vessels is fairly bloodless and allows partial splenectomy. |
Idiopathic thrombocytopenic purpura (ITP) is the most common indication for splenectomy for hematologic diseases. Acute ITP in children younger than 16 years usually responds well to corticosteroids and rarely requires splenectomy. However, in adult patients, splenectomy is usually necessary because of poor response to medical therapy. During the operation, careful exploration, identification, and removal of any accessory spleens is essential in order to prevent recurrence of the disease.
Hereditary spherocytosis responds very well to splenectomy and is the treatment of choice. In other types of anemia, such as thalassemia, sickle cell anemia, or idiopathic autoimmune hemolytic anemia, splenectomy is indicated in symptomatic patients, such as those requiring multiple transfusions, marked splenomegaly, hypersplenism, or repeated splenic infarcts.
Recent evidence supports that splenectomy, with or without central splenorenal shunt, may be beneficial in selected patients with gastroesophageal varices, Child’s B cirrhosis with refractory ascites and splenomegaly, or for reduction of the portal overperfusion in small-for-size graft syndrome in living donor liver transplantation.
Preoperative Preparation
In preparing to perform elective splenectomy, several issues should be considered prior to operation. If the patient has severe splenomegaly, splenic artery embolization may be an adjunct that can reduce operative blood loss and increase ease of removal. In addition, administration of Haemophilus influenza type B, meningococcus, and polyvalent pneumococcal vaccines should be considered 10 to 14 days before splenectomy, in order to reduce the risk of infection by encapsulated organisms. Patients on steroid treatment should have the medication tapered postoperatively over a period of a few days. Patients with myeloproliferative disorders undergoing splenectomy are prone to thrombosis of the splenic and portal vein. Perioperative prophylaxis with low-dose heparin or antiplatelet agents should be considered. In cases with ITP, platelet administration should be considered only after ligation or embolization of the splenic artery in order to prevent their destruction by the spleen.
Laparoscopic splenectomy in the elective setting has been shown to be safe and has the well-documented benefits of minimally invasive techniques. However, there is some evidence that the laparoscopic approach may be associated with a higher incidence of portal venous system thrombosis than the open technique.
Splenic Trauma
The spleen is the most commonly injured intra-abdominal organ following blunt trauma and the second most commonly injured solid organ after penetrating trauma.
Clinical Presentation
The clinical presentation of the patient with an injured spleen depends on the severity of blood loss and the presence of associated injuries. Many patients with isolated low-grade splenic injuries may be asymptomatic or have minor local tenderness and the diagnosis is made by routine ultrasound or CT scan investigations. Some patients may complain of left upper quadrant pain, which might radiate to the left shoulder (Kehr’s sign). In the presence of significant blood loss, the patient may present with signs of hypovolemia, such as tachycardia or hypotension.
Investigations
Routine chest x-ray may be helpful in suspecting splenic injury. The presence of fractures of the left lower ribs should increase the suspicion of splenic trauma, especially in a hypovolemic patient. An elevated left
hemidiaphragm may be indicative of a large splenic hematoma.
hemidiaphragm may be indicative of a large splenic hematoma.
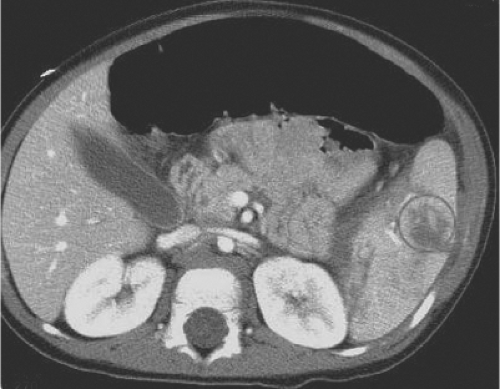 Fig. 4. CT scan shows contrast extravasation (circle), suggestive of active bleeding or false aneurysm. This patient may benefit from angioembolization or operation. |
A trauma ultrasound (FAST) performed by a surgeon or an emergency physician may show free fluid around the spleen. A formal ultrasound may identify the site and extent of the splenic injury.
Abdominal CT scan with intravenous contrast is the most widely used and most reliable investigation in the diagnosis of splenic trauma in hemodynamically stable patients. Besides providing information about the severity and nature of the injury and the amount of intraperitoneal bleeding, it might show evidence of active bleeding (blushing) (Fig. 4) or other associated injuries.
In hemodynamically unstable patients with suspicion of intra-abdominal bleeding, a positive trauma ultrasound should be an indication for an emergency surgery. Alternatively, if ultrasound is not available or the investigation is not conclusive, a diagnostic peritoneal aspirate (DPA) may be valuable in the diagnosis of intra-peritoneal bleeding. The technique of the insertion of the catheter for DPA is exactly the same as with diagnostic peritoneal lavage (DPL). However, after the intra-peritoneal insertion of the catheter, the diagnosis of bleeding is made only by syringe aspiration and without any infusion and lavage with saline. Infusion of fluid in the peritoneal cavity as required with DPL, interferes with the interpretation of subsequent CT scan studies.
Grades of Splenic Injury
Splenic injury can objectively be described with a grading system developed by the American Association for the Surgery of Trauma. The grading is based on the CT scan, operative findings or autopsy findings, and includes five grades (Table 2). Generally, grades I and II are considered minor injuries, grade III as a moderate injury, and grades IV and V as severe injuries (Figs. 5, 6). This grading system standardizes and facilitates comparison of therapeutic modalities and may help in the management (operation or observation) of the injuries. However, although this grading is helpful in deciding the optimal management of the injury, the final decision should be based on the surgeon’s clinical judgment. Many grade III or IV injuries can successfully be managed nonoperatively, especially in the pediatric population. On the other hand, lower-grade injuries sometimes fail nonoperative management.
Table 2 AAST Spleen Injury Scale | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Management
Nonoperative Management
About 80% of blunt splenic injuries in adults and 90% to 95% in children can safely be managed nonoperatively. The selection of patients for nonoperative management is based on clinical examination, CT scan findings, and associated injuries. The patient should be hemodynamically stable, have no signs of peritonitis, and ideally should have no major associated injuries, which may cause coagulopathy and increase the risk of splenic bleeding. Although associated head trauma is not in itself an absolute contraindication to nonoperative management, its presence should lower the threshold for operative intervention, because of the high incidence of head trauma-related coagulopathy, which can be as high as 35%. It is postulated that coagulopathy is caused by massive release of thromboplastin from the injured brain, leading to the activation of the extrinsic clotting cascade.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


