Resonance disorders are commonly seen in a pediatric speech pathology practice. These disorders can be due to a form of velopharyngeal dysfunction (often, but not always, caused by a history of cleft palate) or obstruction in one or more of the cavities of the vocal tract. Occasionally, abnormal resonance can be due to faulty articulation.
The speech-language pathologist (SLP) must make a diagnosis of the type of resonance disorder and probable cause through a focused evaluation of resonance and velopharyngeal function. The differential diagnosis is essential in order to determine appropriate treatment, which may include physical management (surgery or a prosthetic device) and/or speech therapy.
This chapter is intended to be a guide for the practicing clinician who occasionally or frequently sees children with resonance disorders. The chapter begins with a definition and description of how resonance affects voiced sound and speech production. Because the velopharyngeal valve is an important determinant of resonance during speech, normal velopharyngeal function is described. This is followed by a discussion of the common types of resonance disorders and the causes of each. The types and causes of velopharyngeal dysfunction are then discussed. Finally, basic information is given regarding evaluation techniques and appropriate treatment based on the diagnosis of type of resonance and cause.
14.2 Normal Resonance and Velopharyngeal Function
Every instrument that is capable of producing sound has to have at least three components: (1) a vibrating mechanism that can be set in motion to produce sound, (2) a stimulating mechanism that can set the vibration in motion, and (3) a resonating mechanism to reinforce or amplify the sound. In human speech, the vocal folds are the vibrating bodies, the force of air pressure from the lungs is the stimulating force, and the cavities of the vocal tract provide the mechanism for resonance of the sound energy. 1
Resonance, as it relates to speech, is the modification of voiced sound as it travels through the cavities of the vocal tract, which include the pharyngeal cavity, oral cavity, and nasal cavity. Resonance is dependent on two factors—the function of the velopharyngeal valve and the size and shape of the resonating cavities.
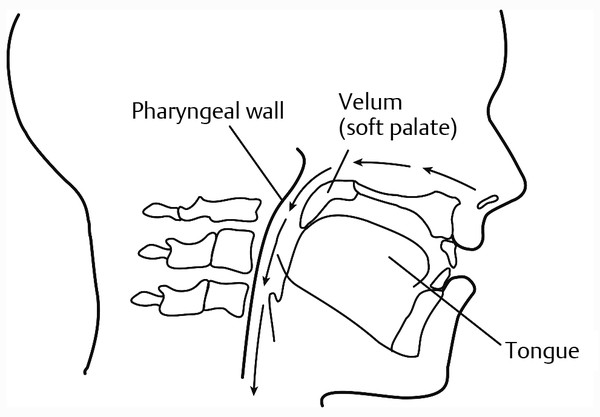
The velopharyngeal valve consists of the velum (soft palate), the lateral pharyngeal walls, and the posterior pharyngeal wall. During nasal breathing, the velum is down and rests against the base of the tongue ( ▶ Fig. 14.1). At the same time, the pharyngeal walls are relaxed. Therefore, the nasopharynx is patent for unobstructed nasal breathing. During speech, however, the velopharyngeal valve opens and closes in order to direct sound energy into the oral or nasal cavity as appropriate for each speech phoneme.
Fig. 14.1 Lateral view of the velum and posterior pharyngeal wall. The velum rests against the base of the tongue during normal nasal breathing, resulting in a patent airway. (From KUMMER. Cleft Palate and Craniofacial Anomalies, 2E. © 2008 Delmar Learning, a part of Cengage Learning, Inc. Reproduced by permission. www.cengage.com/permissions)
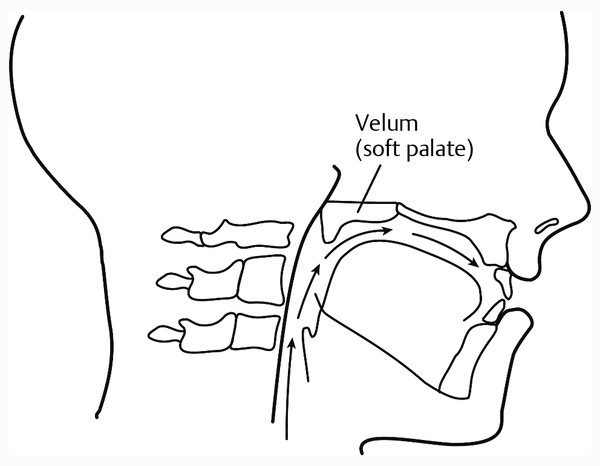
For production of oral phonemes, the velum moves in a superior and posterior direction with a type of “knee action” in order to achieve closure against the pharyngeal walls ( ▶ Fig. 14.2). The posterior pharyngeal wall often moves anteriorly in order to assist in achieving contact. The lateral pharyngeal walls move medially to close against the velum, or in some cases, to meet in the midline behind the velum. Through the coordinated action of these structures, velopharyngeal closure occurs as a valve or sphincter. The closure of this valve serves to direct sound energy into the oral cavity for the oral sounds. For the production of nasal phonemes (/m/, /n/, and /ŋ/), the velopharyngeal valve actively opens to allow sound energy to enter the nasal cavity for nasal resonance.
Fig. 14.2 Lateral view of the velum and posterior pharyngeal wall. The velum elevates during speech and closes against the posterior pharyngeal wall. This allows the air from the lungs and the sound from the larynx to be redirected from a superior direction to an anterior direction to enter the oral cavity for speech. (From KUMMER. Cleft Palate and Craniofacial Anomalies, 2E. © 2008 Delmar Learning, a part of Cengage Learning, Inc. Reproduced by permission. www.cengage.com/permissions)
While the velopharyngeal valve directs sound energy into the appropriate cavity, the size and shape of the cavities determine which formants of the sound are enhanced. As a rule of thumb (and of physics), when complex sound passes through a short or small cavity, the higher frequencies of that sound will be enhanced. In contrast, if the same complex sound passes through a longer or larger cavity, the lower frequencies of that sound will be enhanced. This can be proved by blowing across a bottle that is half full. If you pour out more liquid and blow again, the pitch is now lower. This is because as the bottle is emptied, the resonating cavity of air becomes bigger and, therefore, more of the lower formant frequencies are enhanced. Overall, the size, shape, and configuration of the resonating cavities of the vocal tract result in the unique qualities of each individual’s voice. 1
Resonance is particularly important for the production of vowel sounds. This is because the acoustic properties of each vowel are the result of the size and shape of the oral cavity, as determined by the placement of the speech articulators (tongue, mandible, and lips). Changing the size and shape of the oral cavity through movement of the articulators changes the formant frequencies of the oral sound, resulting in an acoustically different vowel sound. Because vowels are produced by manipulating oral resonance, they are often called “resonance sounds.”
14.3 Resonance Disorders: Types and Causes
Anything that disrupts the transmission of sound through the vocal tract or affects the normal balance of oral and nasal resonance will cause a resonance disorder. Abnormal resonance, therefore, is typically caused by either inadequate function of the velopharyngeal valve or by a blockage in one or more of the resonating cavities. The following is a description of each type of resonance disorder, the typical causes, and appropriate treatment. This information is summarized in ▶ Table 14.1.
Hypernasality | Hyponasality | Cul-de-Sac | Mixed | |
Possible Causes | VPI Palatal fistula Misarticulation if phoneme-specific | Obstruction in nasopharynx or nasal cavity | Obstruction at the exit of a cavity of the vocal tract | VPI and obstruction Apraxia |
Treatment | Usually surgery or prosthesis Speech therapy if phoneme-specific | Medical or surgical treatment | Medical or surgical treatment | Medical or surgical treatment Speech therapy if due to apraxia |
Abbreviation: VPI, velopharyngeal insufficiency/incompetence. | ||||
14.3.1 Hypernasality
Hypernasality is the result of too much sound in the nasal cavity during the production of oral phonemes. It usually occurs as a result of velopharyngeal dysfunction, although it can also be caused by a large oronasal fistula following a cleft palate repair. Hypernasality is particularly perceptible on vowel sounds, which are dependent on oral resonance. Nasalization of oral consonants is also common. For example, an oral voiced plosive (such as /b/) will sound more like its nasal cognate (/m/) when there is hypernasality. Nasalization can also occur on other oral consonants. For example, if there is velopharyngeal insufficiency (abnormal structure of the velopharyngeal valve), the speaker may substitute an /n/ for an /s/ sound as a compensatory strategy. Therefore, with severe hypernasality, connected speech will primarily consist of nasal sounds (/m/, /n/, and /ŋ/).
Hypernasal resonance is often accompanied by nasal air emission during consonant production. The leak of air through the velopharyngeal valve particularly occurs as the speaker attempts to build up oral air pressure for production of pressure-sensitive sounds (plosives, fricatives, and affricates).
A large velopharyngeal opening causes significant nasal emission that is usually inaudible. This is because there is little impedance to the flow, so there is no audible friction. In addition, the sound of hypernasality masks the sound of nasal emission. However, the significant nasal emission causes a loss of intra-oral air pressure. This results in weak or omitted consonants. It also causes short utterance length because more frequent breaths are required to replace the loss of air through the nose.
A lack of adequate intra-oral air pressure for consonant production commonly results in the development of compensatory articulation productions. Common compensatory productions include glottal stops, pharyngeal stops, and pharyngeal fricatives because these sounds can be produced before the airflow is lost through the velopharyngeal valve.
In contrast to a large velopharyngeal opening, a small opening rarely causes hypernasality. However, when air is forced through a small velopharyngeal opening, it is released with a great deal of pressure. This causes audible bubbling of secretions, called a nasal rustle (also called nasal turbulence).
Hypernasality (and even nasal emission) is usually caused by a structural or neurophysiological disorder (see section on velopharyngeal dysfunction). Therefore, treatment almost always requires surgical correction (or a prosthetic device if surgery is not possible or desired). Speech therapy may be required following physical management to correct the compensatory errors.
14.3.2 Hyponasality and Denasality
Hyponasality occurs when there is a reduction of nasal resonance during speech due to a blockage in the nasopharynx or in the entrance to the nasal cavity. A complete occlusion of the nasal cavity during speech results in denasality. Hyponasality and denasality particularly affect the production of the nasal consonants (/m/, /n/, and /ŋ/). When nasal resonance is reduced or eliminated during production of nasal consonants, these consonants sound similar to their oral phoneme cognates (/b/, /d/, and /g/, respectively).
The cause of hyponasality or denasality is almost always obstruction somewhere in the nasopharynx or nasal cavity. (The only exception is when there is apraxia, which can cause the inconsistent substitution of oral sounds for nasal sounds.) This obstruction may be due to adenoid hypertrophy, swelling of the nasal passages secondary to allergic rhinitis, the common cold, a deviated septum, choanal atresia (which is a congenital blockage of the opening into the nasopharynx from the nasal fossa), a stenotic naris, midface deficiency, and others. Because the cause of reduced nasal resonance is strictly obstruction, further evaluation and treatment should be done by a physician.
14.3.3 Cul-de-Sac Resonance
Cul-de-sac resonance occurs when sound is trapped in one of the cavities of the vocal tract due to a blockage at its exit. There are three different types of cul-de-sac resonance, depending on the location of the blockage. Oral cul-de-sac resonance can occur due to microstomia (a small mouth opening). It is also what is heard with “mumbling” or speaking without opening the mouth normally. Nasal cul-de-sac resonance only occurs when there is a combination of velopharyngeal insufficiency and a blockage in the anterior part of the nose. Therefore, it is mostly found in individuals with a history of cleft palate with velopharyngeal insufficiency, and stenotic nares or a deviated septum. Nasal cul-de-sac resonance can be simulated by imitating hypernasality while pinching the nose closed. Pharyngeal cul-de-sac resonance is the most common of the three types. It is typically caused by large tonsils that block sound from entering the oral cavity during speech. This type of resonance has even been described as “potato-in-the-mouth” speech by some authors.
As with hyponasality, cul-de-sac resonance is due to a structural blockage. Therefore, it cannot be corrected with speech therapy. However, the SLP should identify the type and probable cause of the abnormal speech and make a referral for surgical intervention as appropriate.
14.3.4 Mixed Resonance
Mixed resonance occurs when the speech has characteristics of both hypernasality and hyponasality. The hypernasality occurs on oral sounds and the hyponasality occurs on nasal sounds. Mixed resonance is usually due to a combination of velopharyngeal insufficiency and significant nasal airway blockage. In this case, hypernasality is usually the predominate characteristic of connected speech, but hyponasality is noted on the nasal consonants. Mixed resonance can also be caused by apraxia. The motor sequencing problems can affect the timing of the upward or downward movement of the velum, resulting in inappropriate closure or opening of the valve during speech. 2
14.4 Velopharyngeal Dysfunction: Types and Causes
14.4.1 Velopharyngeal Dysfunction
Velopharyngeal dysfunction (VPD) is a condition where the velopharyngeal valve does not close consistently and completely during the production of oral sounds. VPD is used as a broad term that encompasses all disorders (with various causes) that affect closure of the velopharyngeal valve. The following sections describe the various types and causes of velopharyngeal dysfunction and appropriate treatment for each. This information is summarized in ▶ Table 14.2.
Velopharyngeal Insufficiency | Velopharyngeal Incompetence | Velopharyngeal Mislearning | |
Possible causes | Cleft palate Submucous cleft palate Deep pharynx Interference of tonsils S/P adenoidectomy S/P maxillary advancement S/P nasopharyngeal tumor removal | Cerebral palsy Neuromotor diseases/conditions Brainstem tumors Traumatic brain injury CVA Cranial nerve damage | History of VPI Articulation disorder Severe hearing loss or deafness |
Treatment | Surgery or prosthesis and speech therapy as needed | Surgery or prosthesis and speech therapy as needed | Speech therapy |
Abbreviations: CVA, cerebrovascular accident; S/P status post; VPI, velopharyngeal insufficiency/incompetence. | |||
14.4.2 Velopharyngeal Insufficiency
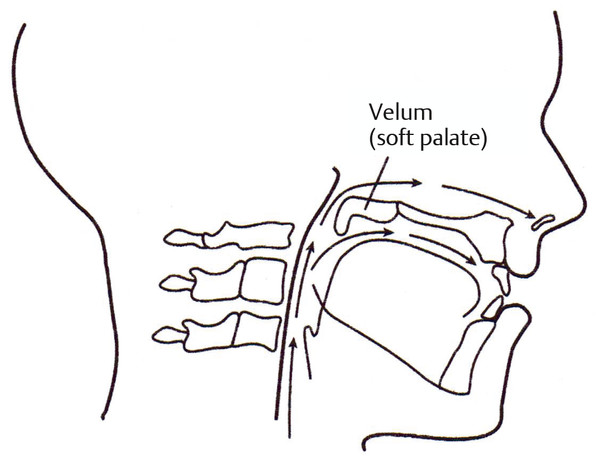
Velopharyngeal insufficiency (VPI) refers to an anatomical or structural defect that prevents adequate velopharyngeal closure. VPI is the most common type of VPD. It can be caused by a short or notched velum, which is common in children with a history of cleft palate, even after palate repair, and also with a submucous cleft palate ( ▶ Fig. 14.3). VPI can even be caused by a deep pharynx secondary to cervical spine or cranial base abnormalities. 3 Even large tonsils can cause VPI if they restrict lateral pharyngeal wall motion or intrude into the nasopharynx to interfere with velopharyngeal closure. 4
Fig. 14.3 Velopharyngeal insufficiency. In this case, the velum is too short to achieve velopharyngeal closure during speech. (From KUMMER. Cleft Palate and Craniofacial Anomalies, 2E. © 2008 Delmar Learning, a part of Cengage Learning, Inc. Reproduced by permission. www.cengage.com/permissions)
VPI may occur after certain types of surgeries, including adenoidectomy, especially if closure was achieved against the adenoid pad or was tenuous from the start. 5 A maxillary advancement procedure to correct midface deficiency can potentially result in VPI because the velum moves anteriorly with the maxilla. 6 Finally, removal of a nasopharyngeal tumor can leave an opening in the palate or affect the velopharyngeal valve. 7
14.4.3 Velopharyngeal Incompetence
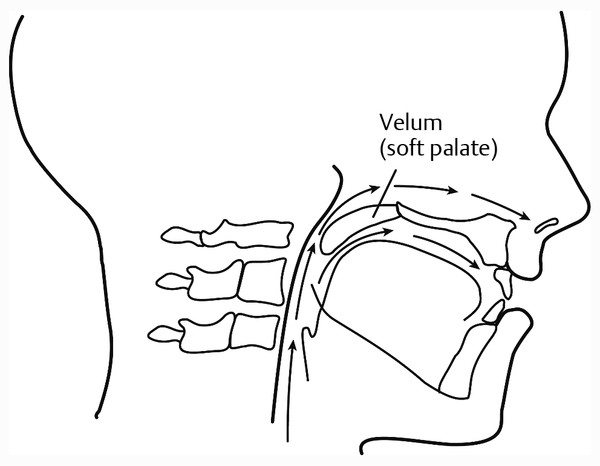
Velopharyngeal incompetence (VPI) refers to a neurophysiological disorder that results in poor movement of the velum and pharyngeal structures ( ▶ Fig. 14.4). Velopharyngeal incompetence can occur in patients with neurological diseases and conditions that cause dysarthria, such as cerebral palsy, myotonic dystrophy, myasthenia gravis, neurofibromatosis, cerebral tumors, traumatic brain injury, and stroke. 8 It can also occur in patients with either congenital or acquired cranial nerve damage. Specific velopharyngeal paralysis or paresis is usually unilateral and can occur in the absence of other motor deficits.
Fig. 14.4 Velopharyngeal incompetence. In this case, the velum does not move well enough to achieve velopharyngeal closure during speech. (From KUMMER. Cleft Palate and Craniofacial Anomalies, 2E. © 2008 Delmar Learning, a part of Cengage Learning, Inc. Reproduced by permission. www.cengage.com/permissions)
14.4.4 Velopharyngeal Mislearning
Velopharyngeal mislearning can cause phoneme-specific hypernasality or nasal air emission. 9 For example, if the patient substitutes a nasal or pharyngeal phoneme for an oral phoneme, the velopharyngeal valve will be open during production, causing nasal emission. Misarticulations that result in phoneme-specific hypernasality include the substitutions of ŋ/l and ŋ/r. Misarticulations that result in phoneme-specific nasal emission include the substitution of a pharyngeal fricative or nasal fricative for sibilant sounds (/s, z, ʃ, ʒ, ʧ, ʤ/).
Velopharyngeal mislearning often occurs with VPI, causing compensatory articulation productions. However, velopharyngeal mislearning can also occur as an isolated articulation disorder in a child with no history of VPI. Finally, velopharyngeal mislearning often occurs in individuals who have severe hearing loss or deafness. In this case, resonance is abnormal due to the lack of auditory feedback, which is required for normal velopharyngeal learning.
The differential diagnosis of type of VPD is of utmost importance because the diagnosis impacts the treatment recommendations. For example, velopharyngeal insufficiency or velopharyngeal incompetence requires physical management (surgery or prosthesis) and often speech therapy after physical management. In contrast, velopharyngeal mislearning is corrected by speech therapy alone.
14.5 Evaluation of Resonance and Velopharyngeal Function
The evaluation of resonance disorders and velopharyngeal function involves a perceptual assessment and oral examination. Depending on the results of those assessments, instrumental procedures may be helpful in further defining the disorders. Assessment procedures are briefly described below and are described elsewhere in more depth. 10, 11, 12, 13
14.5.1 Perceptual Evaluation
For the perceptual speech assessment, it is important to use an appropriate speech sample in order to obtain information that is needed for a definitive diagnosis. Although a formal single-word articulation test is commonly used to assess speech production errors, it is does not provide a good reflection of what occurs in connected speech. In fact, velopharyngeal function, and even articulation, may be normal at the single-word level, but abnormal in connected speech because of the increased demands on the oral-motor system. Therefore, it is far better (and actually much easier) to assess articulation through syllable repetition, counting, and repeated sentences. Using the speech samples described below, the examiner can easily evaluate articulation, airflow, and resonance.
Syllable repetition: Syllable repetition is a fast and easy way to assess articulation, resonance and the presence of nasal emission. The child is asked to produce all the consonants in a repetitive manner (i.e., /pɑ pɑ pɑ pɑ pɑ/; /pi pi pi pi pi/; /tɑ tɑ tɑ tɑ tɑ/; /ti ti ti ti ti/, etc.). Particular attention should be paid to pressure-sensitive phonemes (plosives, fricatives, and affricates), which may be produced with nasal emission or substituted by a compensatory production. All consonant phonemes should be tested with both a low vowel (i.e., /ɑ/) and then again with a high vowel (i.e., /i/). High vowels are more sensitive to hypernasality. 14 The repetition of the syllables mimics the oral-motor demands of connected speech, while allowing the examiner to focus on only one consonant and one vowel at a time. This procedure makes it easy to determine if there is phoneme-specific nasal air emission on sibilants (i.e., /s, z, ʃ, ʒ, ʧ, ʤ/) or phoneme-specific hypernasality on high vowels (i.e., /i/).
Counting: Counting can also provide the examiner with a fast, easy, and reliable test. A good test of hypernasality and/or nasal emission is counting from 60 to 70 or repeating either the numbers 60 or 66 over and over. The number 66 is particularly good to use because it contains several /s/ sounds, the high vowel (/i/) and several /s/ blends (/kst/ and /ks/). To test for hyponasality, counting from 90 to 99 allows the examiner to assess the production of the nasal /n/ in connected speech.
Sentence Repetition: By asking the patient to repeat certain sentences, the examiner can quickly and easily assess articulation, nasal emission, and even resonance in a connected speech environment. This is much faster than a single-word articulation test, less expensive because there is nothing to buy, and is actually a more valid test of normal speech production than a formal articulation test.
For this part of the assessment, it is preferable to use sentences that contain phonemes that are similar in articulatory placement so that one type of speech sound is evaluated in each sentence. A few sample sentences are as follows:
t Take teddy to town
d Do it for daddy
g Go get the cookie
f Fred has five fish
s Sissy sees the sun in the sky.
z I saw a zebra at the zoo.
ʃ She went shopping.
ʧ I eat cherries and cheese.
j John told a joke to Jim.
m My name is Mary.
Articulation and Airflow
In any speech assessment, the examiner determines if there are misarticulations (errors of articulation placement) that are not developmental in nature. When there are structural abnormalities, the examiner must also determine if there are compensatory errors or obligatory distortions.
Compensatory errors are misarticulations that occur in an effort to improve intelligibility of speech by altering placement in response to the abnormal structure. With significant VPI, the speaker may compensate for the lack of oral airflow by moving the placement of oral sounds to the pharynx where there is airflow. This can result in the use of glottal stops, pharyngeal plosives, pharyngeal fricatives, and posterior nasal fricatives as substitutions for oral pressure sounds.
Structural abnormalities, including VPI, can also cause obligatory distortions. Obligatory distortions are characterized by an abnormal acoustic product due to a structural abnormality, despite normal articulatory placement. For example, if articulation placement is normal but there is a large velopharyngeal opening during speech, plosives will be heard as their nasal cognates (i.e., m/b, n/d, ŋ/g). Hypernasality and nasal emission with normal articulation placement are also obligatory distortions. It should be noted that because obligatory distortions are due to abnormal structure and not abnormal function, they cannot be corrected with speech therapy. Instead, physical correction of the structure is needed.
In addition to speech sound production, the examiner should note the occurrence of audible nasal air emission (including nasal rustle) during the production of pressure-sensitive phonemes.
The consistency of nasal air emission should be observed. It is particularly important to note if the nasal emission always occurs on certain phonemes (such as /s/ or all sibilants), but not on other pressure-sensitive sounds. If consonants are weak in intensity and pressure, it can be assumed that inaudible nasal emission is the cause.
Assessing stimulability is an important component of the evaluation. If there is an elimination of nasal emission with a change in articulatory placement, this suggests that the nasal emission is due to faulty articulation in the pharynx. Therefore, this is a good prognostic indicator for correction with therapy. If there is nasal emission despite normal placement, this suggests that the cause is VPI, which requires physical management.
Resonance
If there is abnormal resonance, it is very important to determine the type of resonance because the type is what determines appropriate treatment. Some clinicians also rate the severity of the abnormal resonance by using numeric scales (i.e., 1 through 7) or descriptive scales (i.e., mild, moderate, severe). Fortunately, the severity rarely has an impact on treatment, so rating severity is not essential.
Resonance should be judged by listening to the quality of the vowels, which are particularly affected by hypernasality. In addition, there may be a predominance of nasal consonants in connected speech. Hypernasality is often more apparent in connected speech than in single words or short utterances because connected speech increases the demands on the velopharyngeal valving system to achieve and maintain closure.
With hyponasality and cul-de-sac resonance, the vowel may be slightly affected, but distortion of nasal phonemes will be most noticeable. A muffled sound with low volume will often indicate cul-de-sac resonance.
Supplemental Tests
Experienced clinicians are usually able to reliably evaluate the resonance and velopharyngeal function by merely listening to the patient’s speech. However, less experienced clinicians may find it helpful to employ some supplemental tests to more clearly define the speech and resonance characteristics and to determine the potential cause.
The following are some simple “no tech” devices and evaluation procedures that may be useful.
Listening Tube: A plastic “listening tube” is a great tool for evaluation of resonance and velopharyngeal function. A piece of suction tubing or a long plastic whistle can be used for this purpose. Even a stethoscope can be used as a listening tube by taking the drum off the end. When using a listening tube, one end of the tube is placed in the child’s nostril and the other end is placed near the examiner’s ear ( ▶ Fig. 14.5). To evaluate for hypernasality, the patient repeats words or sentences devoid of nasal consonants. Even if there is slight hypernasality or nasal emission, this will be heard loudly through the tube. To evaluate for hyponasality, the patient is asked to produce nasal sounds or prolong an /m/. If little to no sound is heard through the tube, this indicates obstruction and confirms hyponasality, and in some cases, cul-de-sac resonance.
Straw: A straw is the ultimate low cost, low-tech instrument; yet, it is extremely helpful and reliable in evaluating resonance and detecting nasal emission. By placing the short end of the bending straw in the child’s nostril and the other end near the examiner’s ear, the examiner can detect even slight hypernasality or nasal emission in the same way as with a the listening tube ( ▶ Fig. 14.6). Again, hyponasality is tested by having the patient produce nasal sounds. A straw has certain distinct advantages over a tube. A straw is readily available in most settings, costs less than a penny, and is disposable.
Cul-de-Sac Test: The cul-de-sac test can be used to confirm the presence of hypernasality. With this informal test, the child is asked to produce a vowel or repeat a sentence that is completely devoid of nasal consonants. The child then repeats the same utterance with the nares occluded. In normal speech, there should be no perceptible difference in the quality of the production because the nasal cavity is already closed by the velopharyngeal valve. If there is a difference in quality with closure of the nasal cavity at the nares, this suggests hypernasality due to VPI. If resonance is perceived as abnormal, but closure of the nares results in no change in quality, this suggests either cul-de-sac resonance or hyponasality.
Fistula Test: To determine if a fistula is the cause of nasal air emission, the examiner should determine if there is a difference in the degree of nasality for anterior sounds (/p/, /t/, /s/) versus the posterior sound /k/. More nasality on anterior sounds than the /k/ sound suggests a symptomatic anterior oronasal fistula.
Fig. 14.5 A “listening tube” for a test of nasal air emission and hypernasality. One end of a plastic tube is placed in the child’s nostril or at the entrance to the nostril, and the other end is placed in the examiner’s ear. As the child produces sounds or sentences, the examiner can hear occurrences of nasal air emission or hypernasality. (From KUMMER. Cleft Palate and Craniofacial Anomalies, 2E. © 2008 Delmar Learning, a part of Cengage Learning, Inc. Reproduced by permission. www.cengage.com/permissions)


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


