CHAPTER 27 Intracranial region
The cranial cavity contains the brain, the intracranial portions of cranial and spinal nerves, blood vessels, meninges and cerebrospinal fluid. Its walls are formed by parts of the frontal, ethmoid, parietal, sphenoid, temporal and occipital bones.
INTERNAL SURFACE OF CRANIAL VAULT
The internal surface of the cranial vault is deeply concave. It includes most of the frontal and parietal bones and the squamous part of the occipital bone, variously united at the coronal, sagittal and lambdoid sutures (Fig. 27.1). With increasing age, these sutures become obliterated by a gradual process that begins on their intracranial surfaces. Inconstant foramina may occur in the parietal bones near the sagittal sulcus and anterior to the lambdoid suture: they admit emissary veins associated with the superior sagittal sinus. The internal surfaces of the frontal and parietal bones are grooved by furrows that house the frontal and parietal branches of the middle meningeal vessels; the grooves contain the openings of minute channels that admit perforating vessels to the haemopoietic marrow within the diploic bone. Impressions for cerebral gyri are less distinct on the vault than they are on the cranial base.

CRANIAL FOSSAE (ANTERIOR, MIDDLE, POSTERIOR)
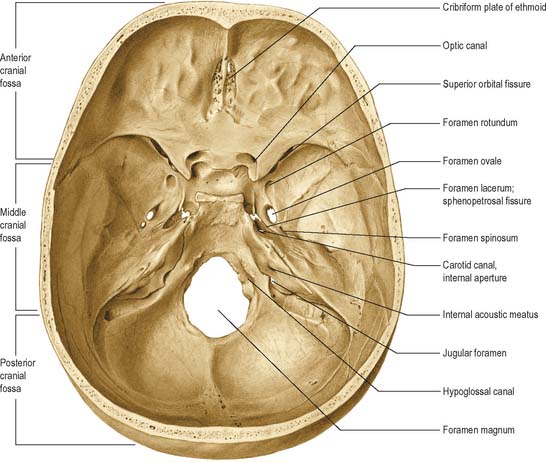
The base of the cranial cavity is divided into three distinct fossae, the anterior, middle and posterior cranial fossae (Fig. 27.2). The floor of the anterior cranial fossa is at the highest level and the floor of the posterior fossa is at the lowest.
ANTERIOR CRANIAL FOSSA
The convex cranial surface of the frontal bone separates the brain from the orbit and bears impressions of cerebral gyri and small grooves for meningeal vessels. Posteriorly, it articulates with the anterior border of the lesser wing of the sphenoid bone which forms the posterior boundary of the anterior cranial fossa. The medial end of the lesser wing constitutes the anterior clinoid process. The lesser wing joins the body of the sphenoid body by two roots which are separated by the optic canal. The anterior root, broad and flat, is continuous with the jugum sphenoidale, while the smaller and thicker posterior root joins the body of the sphenoid bone near the posterior bank of the sulcus chiasmatis. The frontosphenoid and sphenoethmoidal sutures divide the sphenoid from the adjacent bones.
MIDDLE CRANIAL FOSSA
The middle cranial fossa communicates with the orbits by the superior orbital fissures, each bounded above by a lesser wing, below by a greater wing, and medially by the body of the sphenoid bone. The fissures are wider medially, and each has a long axis sloping inferomedially and forwards. They are the major gateways into the orbit from the cranial cavity and contain the oculomotor, trochlear and abducens nerves, and the lacrimal, frontal and nasociliary branches of the ophthalmic division of the trigeminal nerve, together with filaments from the internal carotid plexus (sympathetic), the ophthalmic veins, the orbital branch of the middle meningeal artery, and the recurrent branch of the lacrimal artery (see Ch. 39).
Centrally the floor of the fossa is narrower and formed by the body of the sphenoid bone which contains the sphenoidal sinuses (see Ch. 32). The roof of the sinus is deeply concave and houses the pituitary gland (hypophysis): it is therefore termed the pituitary (hypophysial) fossa, also known as the sella turcica because it resembles the shape of a Turkish saddle. The anterior edge of the pituitary fossa is completed laterally by a middle clinoid process, the floor forms the roof of the sphenoidal air sinuses, and the posterior boundary presents a vertical pillar of bone, the dorsum sellae. The superolateral angles of the dorsum are expanded as the posterior clinoid processes. A fold of dura, the diaphragma sella, is attached to the anterior and posterior clinoid processes and roofs over the pituitary fossa. The smooth upper part of the anterior wall of the fossa, the jugum sphenoidale, is bounded behind by the anterior border of the grooved sulcus chiasmatis which leads laterally into the optic canals. Each canal transmits the optic nerve and ophthalmic artery. The optic chiasma usually lies posterosuperior to the sulcus chiasmatis, the tuberculum sellae lies below the sulcus. The cavernous sinus lies lateral to the pituitary fossa. The lateral wall of the body of the sphenoid contains a shallow carotid groove related to the internal carotid artery as it ascends from the carotid canal and runs through the cavernous sinus. Posterolaterally the groove may be deepened by a small projecting lingula.
The trigeminal impression, which accommodates the trigeminal ganglion, is situated posterior to the foramen lacerum on the anterior surface of the petrous part of the temporal bone near its apex. Its depth is variable. Posterolateral to the impression is a small, shallow, pit, limited posteriorly by a rounded arcuate eminence (produced by the underlying anterior semicircular canal). Lateral to the impression a narrow groove passes posterolaterally into the hiatus for the greater petrosal nerve, and even further laterally is the hiatus for the lesser petrosal nerve. A smooth trigeminal notch leads into the impression. It lies on the upper border of the petrous temporal, anteromedial to the groove for the superior petrosal sinus; at this point, the trigeminal nerve separates the sinus from bone. At the anterior end of the trigeminal notch is the petrosphenoidal ligament (of Gruber), attached to a minute bony spicule, directed anteromedially. The abducens nerve bends sharply across the upper petrous border, and passes between the ligament and the dorsum sellae anterior to the petrosphenoidal ligament (for a detailed analysis of the course of the abducens nerve in the petroclival region see Ozveren et al 2002).
POSTERIOR CRANIAL FOSSA
The hypoglossal (anterior condylar) canal lies medial to and below the lower border of the jugular foramen, at the junction of the basilar and lateral parts of the occipital bone. It transmits the hypoglossal nerve and its recurrent branch together with the meningeal branch of the ascending pharyngeal artery and an emissary vein which links the (intracranial) basilar plexus with the (extracranial) internal jugular vein. When a posterior condylar canal is present behind the occipital condyle, its internal orifice is posterolateral to that of the hypoglossal canal and it contains a sigmoid emissary vein (associated with the occipital veins) and a meningeal branch of the occipital artery. The occipital condyles lie within the anterior aspect of the foramen magnum: their medial aspects are roughened for the attachments of the alar ligaments associated with the atlanto-axial joints.
MENINGES
Cranial and spinal meninges are continuous through the foramen magnum. The cranial meninges are described in this section and the spinal meninges are described on p. 751).
DURA MATER
The cranial dura, which lines the cranial cavity, differs from the spinal dura mainly in its relationship to the surrounding bones. It has an inner, or meningeal, layer and an outer, or endosteal, layer. These layers are united except where they separate to enclose the venous sinuses that drain blood from the brain. There is little histological difference between the endosteal and meningeal layers. Both contain fibroblasts, and the endosteal layer also contains osteoblasts. Focal calcification may occur in the falx cerebri.
Dural partitions
Falx cerebri
The falx cerebri is a strong, crescent-shaped sheet that lies in the sagittal plane and occupies the longitudinal fissure between the two cerebral hemispheres (Fig. 27.3). The crescent is narrow in front, where the falx is fixed to the crista galli, and broad behind, where it blends with the tentorium cerebelli: the straight sinus runs along this line of attachment (Fig. 27.3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


