Surgery of the Liver, Biliary Tract, Pancreas, and Spleen
LEARNING OBJECTIVES
After studying this chapter the reader will be able to:
• Identify the anatomy of the hepatobiliary system
• Correlate physiologic conditions of the hepatobiliary system with surgical interventions
• Discuss procedural considerations for select hepatobiliary surgical interventions
• Compare diagnostic methods for determining surgical interventions and/or approaches
• List five steps to protect patients with a latex allergy or sensitivity
• List the three main steps of Universal Protocol
• List four pharmacologic/hemostatic agents utilized during biliary surgery and describe how they work
• Discuss types of hepatobiliary procedures
• List the two most common diseases of the biliary tree
• Contrast the advantages and disadvantages of laparoscopic and robotic-assisted surgery
• List the supplies needed for a cholangiogram and describe the procedural steps
• List the three types of pancreatic transplant
• List four common postoperative complications of liver transplants
Overview
A pathologic condition in the liver, biliary tract, pancreas, or spleen often requires surgical intervention. These organs are highly vascular and control many metabolic and immune functions of the body. Surgical intervention may be indicated for infection, cystic anomalies, congenital anomalies, metabolic diseases, trauma (see Chapter 18), or malignancy. Many new cases of malignancy of the pancreas, gallbladder, or extrahepatic biliary tract are diagnosed each year and the prognosis for these is often poor (Steer, 2008; Chari and Shah, 2008). Pancreatic cancer remains the fourth leading cause of death in the United States (McPhee et al, 2007). In the past decade, surgeries of the liver and biliary tract have become more advanced as research and new technology permit more complete diagnoses of pathologic conditions. A resection of the liver for carcinoma has achieved a recognized role for cure or substantial palliation with safety and low morbidity.
Cholecystectomy is the most common, nonemergency abdominal operation performed. In the United States more than 750,000 cholecystectomies are performed each year. It is one of the most frequently performed inpatient procedures in the United States (Afdhal and Vollmer, 2008; Chari and Shah, 2008). Laparoscopic cholecystectomy has become the gold standard surgical intervention for the treatment of cholecystitis. Since the early 1990s, laparoscopic cholecystectomy, as compared with open-incision cholecystectomy, has resulted in reduced trauma to tissues as well as shorter postoperative recoveries, both distinct advantages. About 94% of cholecystectomies are elective surgeries while the remainder are emergencies (Afdhal and Vollmer, 2008). Laparoscopic cholecystectomies were the precursor to numerous abdominal procedures now performed or assisted with the laparoscope. Current innovations in cholecystectomy are focusing on removal of the gallbladder through a natural orifice (referred to as NOTES, or natural-orifice transluminal endoscopic surgery) (Ramos et al, 2008).
Solid Organ Transplant
In the eighteenth century, researchers experimented with solid organ transplants on animals and humans. Transplant science evolved after many trials and failures. Important medical breakthroughs, such as surgical technique, tissue typing, immunology, immunosuppressant drugs, and organ preservation, have permitted more success in the viability of organs and longer survival rates for transplant recipients. The following is a summarized timeline of significant “firsts” and milestones in the evolution of solid organ transplant surgery, an often clinically effective and life-saving strategy for patients with end-stage organ failure.
Boston doctors perform face transplant, available at www.cbsnews.com/stories/2009/04/10/health/main4934319.shtml?source=RSSattr=HOME_4934319.
Accessed April 15, 2009; History of transplantation timeline, available at www.organtransplants.org/understanding/history. Accessed April 1, 2009; Linden PK: History of solid organ transplantation and organ donation, Crit Care Clin 25(1), 2009; Milestones in transplantation data, available at www.unos.org/data/default.asp?display=liver&displayType=internationalData. Accessed April 1, 2009; Saudi surgeons perform. rst uterus transplant, 2002, available at www.nytimes.com/2002/03/07/world/medical-first-a-transplant-of-a-uterus.html?sec=health-42k. Accessed April 1, 2009.
New diagnostic technology and the intraoperative use of ultrasonography, biliary endoscopy, and radiography have enabled surgeons to better treat diseases of the biliary tract. Solid organ transplantation (History box), such as for the liver, pancreas, and kidneys, has become common as a means to treat primary hepatic tumors, end-stage liver disease, and insulin-deficient diabetes. Liver transplant procedures have advanced to include entire organ transplants as well as living-related organ donations.
This chapter explores the most common open and minimally invasive procedures performed on the liver, biliary tract, pancreas, and spleen.
Surgical Anatomy
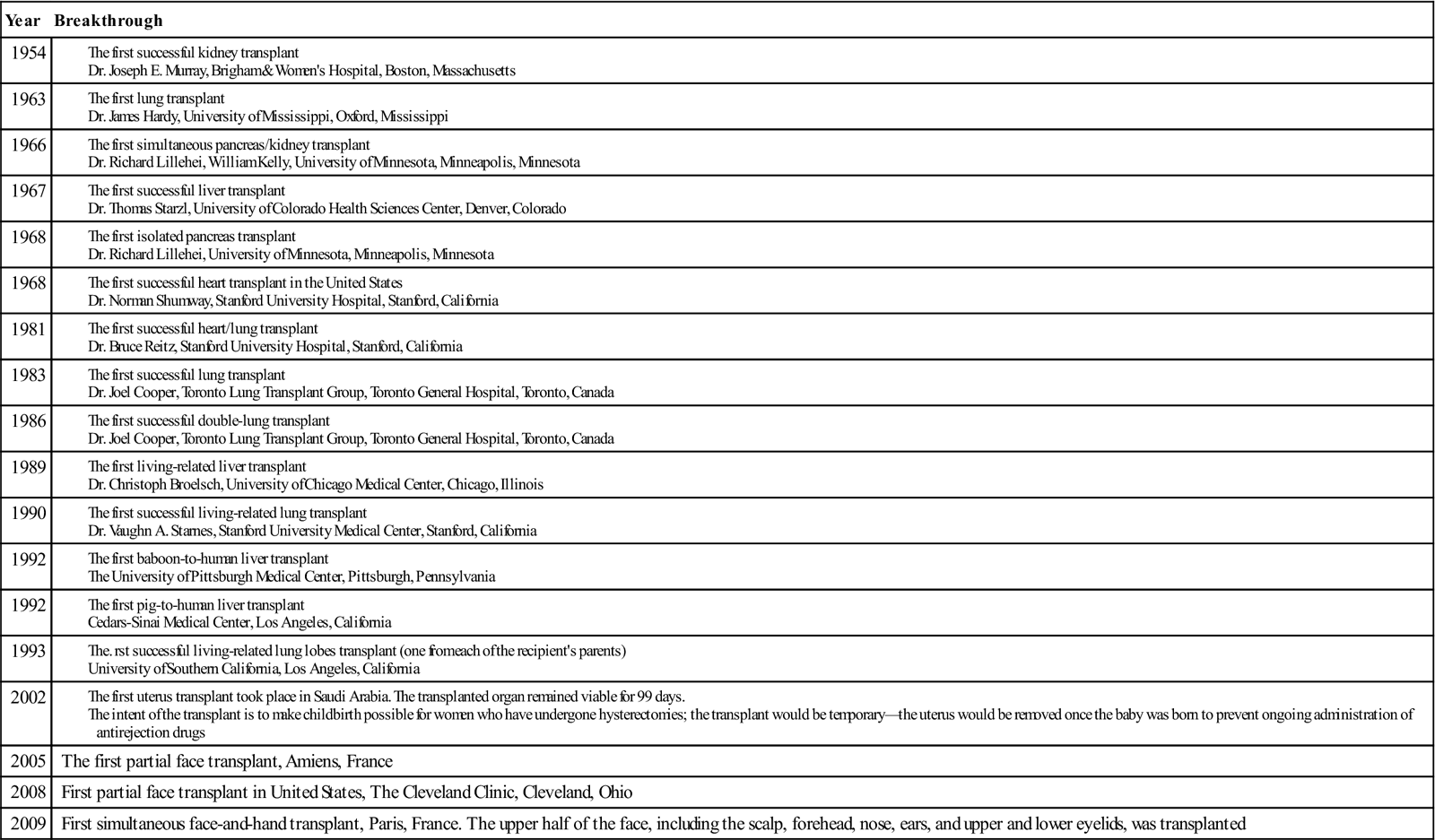
The liver is in the right upper quadrant of the abdominal cavity, beneath the dome of the diaphragm and directly above the stomach, duodenum, and hepatic flexure of the colon. The external covering, known as Glisson’s capsule, is composed of dense connective tissue. The visceral peritoneum extends over the entire surface of the liver, except at the point of posterior attachment to the diaphragm. This connective tissue branches at the porta hepatis into a network of septa that extends into an intrahepatic network of support for the more than 1 million hepatic lobules. The porta hepatis is located on the inferior surface of the liver and provides entry and exit for the major vessels, ducts, and nerves. The hepatic artery maintains the arterial blood supply, while venous blood from the stomach, intestines, spleen, and pancreas travels to the liver by the portal vein and its branches (Figure 3-1). The hepatic venous system returns blood to the heart via the inferior vena cava.
Lobules are the functional units of the liver. Each lobule contains a portal triad that consists of a hepatic duct, a hepatic portal vein branch, and a branch of the hepatic artery, nerves, and lymphatics. A central vein is located in the center of each lobule and provides venous drainage into the hepatic veins.
Lobules also contain hepatic cords, hepatic sinusoids, and bile canaliculi. The hepatic cords consist of numerous columns of hepatocytes—the functional cells of the liver. The hepatic sinusoids are the blood channels that communicate among the columns of hepatocytes. The sinusoids have a thin epithelial lining composed primarily of Kupffer cells—phagocytic cells that engulf bacteria and toxins. The sinusoids drain into the central vein.
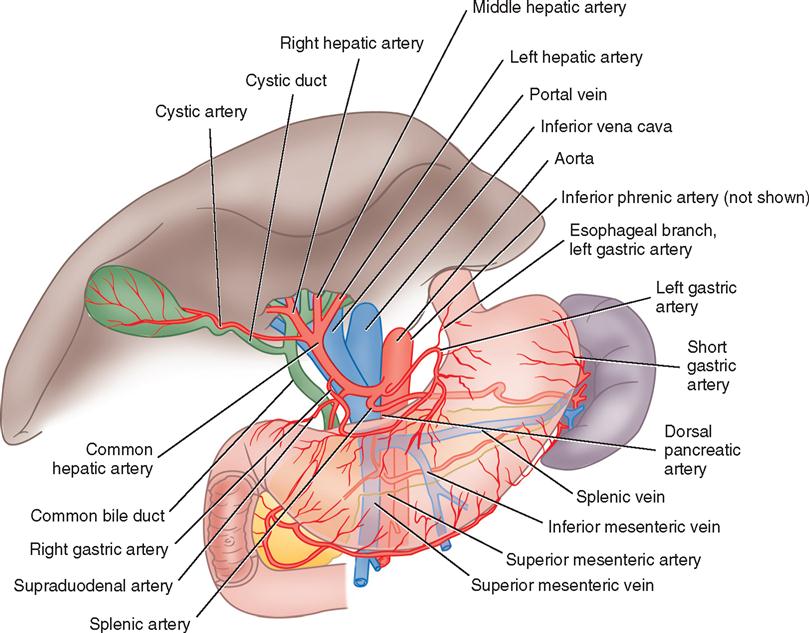
Bile is manufactured by the hepatocytes. The bile canaliculi are tiny bile capillary vessels that communicate among the columns of hepatocytes. The bile canaliculi collect and transport bile to the bile ducts in the portal triad of each lobule, from which bile then flows into the hepatic ducts at the porta hepatis. These ducts join immediately to form one common hepatic duct that merges with the cystic duct from the gallbladder to form the common bile duct (Figure 3-2). The common bile duct opens into the duodenum in an area called the ampulla, or papilla of Vater, located about 7.5 cm below the pyloric opening from the stomach.
Bile contains bile salts, which facilitate digestion and absorption, and various waste products. The liver is essential in the metabolism of carbohydrates, proteins, and fats. It metabolizes nutrients into stores of glycogen, used for regulation of blood glucose levels and as energy sources for the brain and body functions.
The liver plays several important roles in the blood-clotting mechanism. It is the organ that synthesizes plasma proteins, excluding gamma globulins but including prothrombin and fibrinogen. Vitamin K, a co-factor to the synthesis of prothrombin, is absorbed by the metabolism of fats in the intestinal tract as a result of bile formation by the liver. Patients with liver disease may have altered blood-coagulation abilities.
The liver also synthesizes lipoproteins and cholesterol. Cholesterol is an essential component of the blood plasma. It serves as a precursor for bile salts, steroid hormones, plasma membranes, and other specialized molecules. A diet high in cholesterol reduces the amount that must be synthesized by the liver. When the diet is deficient in cholesterol, the liver increases synthesis to maintain levels necessary for production of vital chemical molecules.
The liver also serves in the metabolic alteration of foreign molecules or biotransformation of chemicals. The microsomal enzyme system (MES) plays a major role in the body’s response to foreign chemicals, such as pollutants, drugs, and alcohol. Patients with liver disease may have an altered response to chemical substances. This consideration is important in the induction and management of general anesthesia for patients with liver disorders.
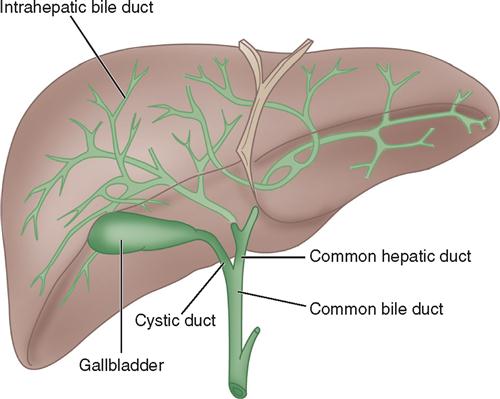
The gallbladder, which lies in a sulcus on the undersurface of the right lobe of the liver, terminates in the cystic duct (Figure 3-3). This ductal system provides a channel for the flow of bile to the gallbladder, where it becomes highly concentrated during storage. The liver produces about 600 to 1000 ml of bile each day. The gallbladder’s average storage capacity is 40 to 70 ml. As foods, especially fats, are ingested, the duodenal cells release cholecystokinin. As the musculature of the gallbladder contracts, bile is forced into the cystic duct and through the common duct. As the sphincter of Oddi in the ampulla of Vater relaxes, bile is released, flowing into the duodenum to aid in digestion by emulsification of fats. The gallbladder receives its blood supply from the cystic artery, a branch of the hepatic artery. The triangle of Calot contains the cystic artery (and possibly the right hepatic artery); it is an anatomic landmark in surgical removal of the gallbladder. Its boundaries may be remembered as “the 3 Cs”: Cystic duct, Common hepatic duct, and Cystic artery (Chari and Shah, 2008). Innervation for the gallbladder and biliary tree is controlled by the autonomic nervous system. Parasympathetic innervation stimulates contraction, whereas sympathetic innervation inhibits contraction.
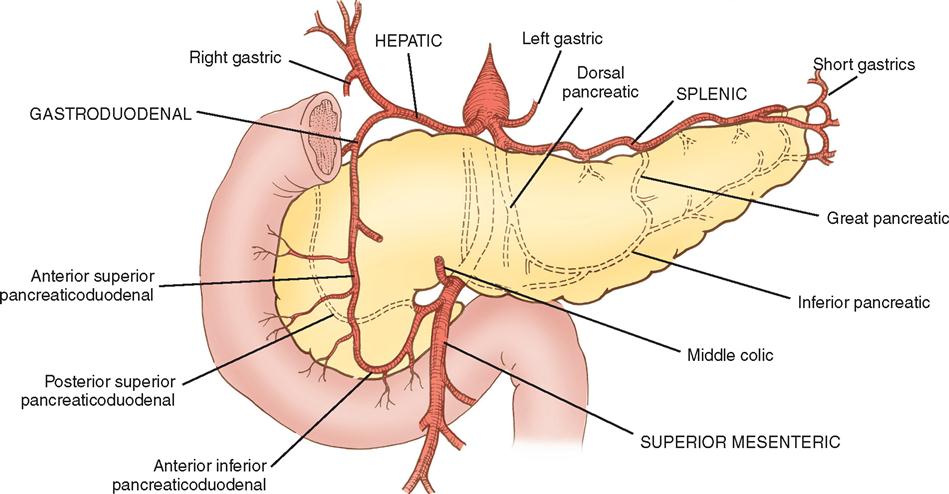
The pancreas (see Figure 3-3) is a fixed structure lying transversely behind the stomach in the upper abdomen. The head of the pancreas is fixed to the curve of the duodenum. Blood is supplied to the pancreas and the duodenum from the celiac axis and superior mesenteric artery (Figure 3-4). The body of the pancreas lies across the vertebrae and over the superior mesenteric artery and vein. The tail of the pancreas extends to the hilum of the spleen. In total, the pancreas extends about 25 cm. Pancreatic secretions containing digestive enzymes are collected in the pancreatic duct, or duct of Wirsung, which joins with the common bile duct to enter the duodenum about 7.5 cm below the pylorus. The dilated junction of the two ducts at the point of entry forms the ampulla of Vater.
The pancreas also contains groups of cells, called islets, or islands, of Langerhans, that secrete hormones into the blood capillaries instead of into the duct. These hormones are insulin and glucagon, and both are involved in carbohydrate metabolism.
Monitoring Mycophenolic Acid: A Method to Detect Rejection in Solid Organ Transplants
Although solid organ transplants are commonly performed, complications occur, the most common and significant being infection and acute graft rejection. In light of the significance of rejection, this review sought evidence for the utility of monitoring concentrations of mycophenolic acid (MPA) in patients who receive solid organ transplants to answer three questions: (1) if such monitoring resulted in a lower incidence of transplant rejections and adverse events versus no monitoring of MPA; (2) whether the incidence of rejection or adverse events differs according to dose, frequency, type of MPA, the form of MPA monitored, the method of MPA monitoring, or sample characteristics; and (3) whether such monitoring is cost-effective. A number of database searches were conducted. Each of the studies selected from the database search was abstracted according to select criteria, two of which were study design (i.e., randomized, controlled trial [RCT], observational study with comparison group, or case series) and patient receipt of allograft solid organ transplant. To be included in the search for evidence, any form of MPA had to be measured in the study at least once (plasma or serum, using any method of measurement). MPA measurement needed to be linked in the study to transplant rejection.
The results were inconclusive in providing evidence for clinical practice. While the state of knowledge about therapeutic drug monitoring of MPA in solid organ transplants remains in its infancy, clinicians are advised to make monitoring decisions on a patient-by-patient basis.
Modified from Utility of monitoring mycophenolic acid in solid organ transplant patients, Feb 2008, available at www.ahrq.gov/clinic/tp/mpaorgtp.htm. Accessed April 1, 2009.
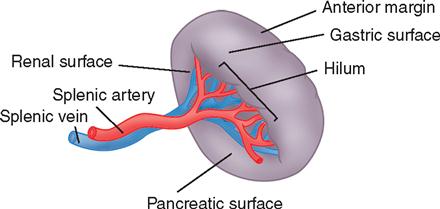
The spleen (Figure 3-5) is in the upper left abdominal cavity, with full protection provided by the tenth, eleventh, and twelfth ribs; its lateral surface is directly beneath the dome of the diaphragm. The anterior medial surface is in proximity to the cardiac end of the stomach and the splenic flexure of the colon. The spleen is covered with peritoneum that forms supporting ligaments. The splenic artery, a branch of the celiac axis, furnishes the arterial blood supply. The splenic vein drains into the portal system.
The spleen has many functions. Among them are defense of the body by phagocytosis of microorganisms, formation of nongranular leukocytes and plasma cells, and phagocytosis of damaged red blood cells. It also acts as a blood reservoir.
Surgical Technologist Considerations
Hepatobiliary surgery is a demanding surgical specialty. The anatomic structures are delicate and surrounded by major blood vessels. It is important the surgical technologist be aware of the procedure, anatomy involved, surgeon’s preferences, and any unique items that may be needed for each patient. Special care needs to be paid to the potential for significant blood loss. It is imperative the surgical technologist have the required items at the ready. In the event of major blood loss, vascular instruments, sutures, and hemostatic agents may be required in rapid succession.
Laparoscopic surgery and the emerging field of robotic procedures can bring a sense of simplicity to the surgery. However, the risk of bleeding or a bile duct injury can still occur. In these instances, it is vital the surgical technologist be able to rapidly convert the procedure to an open procedure. In this event maintaining the sterile field, counting multiple instrument pans, receiving medications onto the sterile field, and communicating with the surgical team must be done with the utmost accuracy. The surgical technologist needs to be aware of any patient allergies, because this may affect the medications received onto the sterile field. It is also important to keep an accurate record of irrigation used. This will help the surgical team determine the estimated blood loss.
Another vital area of importance is specimen labeling. In any large abdominal procedure multiple specimens may be received for pathology. Verification of the surgical specimen, the medium that it should be placed in, and how it will be sent to pathology are critical to obtaining a correct pathology result. Some specimens will be sent to pathology for freezing to determine if margins are clear. The surgical technologist plays a key role in this process. Specimens that are mislabeled or mishandled could affect the patient’s treatment during surgery, as well as postoperatively.
Interventions
Implementation
Patients having surgery of the liver, biliary tract, pancreas, or spleen are usually given a general anesthetic. The following pertinent factors should be considered in caring for these patients.
Universal Protocol.
The Joint Commission (TJC) requires that the “wrong site, wrong procedure, wrong person” prevention protocol be carried out before each surgical procedure (TJC, 2009). This protocol involves the following principles:
♦ Wrong site, wrong procedure, wrong person surgery can and must be prevented.
♦ Active involvement and effective communication among all members of the surgical team are required.
♦ The patient (to the extent possible) should be involved in the process.
♦ Consistent implementation is necessary.
♦ The protocol is flexible to allow for implementation with adaptation to patient needs.
♦ The protocol is adaptable to all procedures that expose patients to the risk for harm.
Proper implementation of the Universal Protocol should use the following steps:
♦ The signed consent should have the correct site and specific procedure documented.
♦ The surgical posting should match the procedure.
3. “Time-out” immediately before starting the procedure (the final verification of the correct patient, procedure, and site).
Positioning the Patient.
For biliary surgery, the patient is placed in supine position. Arms are placed on padded armboards with the palms up and fingers extended. Armboards are maintained at less than a 90-degree angle to prevent brachial plexus stretch. If there are surgical reasons to tuck the arms at the side, the elbows are padded to protect the ulnar nerve, the palms face inward, and the wrist is maintained in a neutral position (Denholm, 2009). A drape secures the arms. It should be tucked snuggly, but not tightly, under the patient, not under the mattress. This prevents the arm from shifting downward intraoperatively and resting against the OR bed rail. A small positioning aid may be placed under the lower right side of the thorax to elevate the lower rib cage, providing better exposure and access to the viscera in the right upper quadrant of the abdomen. Alternatively, a lateral tilt of the OR bed may be used in combination with reverse Trendelenburg for procedures such as laparoscopic cholecystectomy.
Positioning for laparoscopic procedures requires caution when applying safety straps. Given that the patient may be placed in a severe side tilt or reverse Trendelenburg position, safety or restraining straps must be placed securely, but not too tightly. Attention is given to proper alignment of the patient’s body and extremities, and padded footboards are applied to prevent the patient from slipping. Areas of pressure in the selected surgical position and bony prominences are padded well to prevent interruption of circulation and pressure injury to tissues and neurovascular structures. These precautions are especially important for diabetic, circulatory-impaired, immunocompromised, and elderly patients. Close monitoring of the patient is essential during positional changes, especially in laparoscopic procedures with decreased lighting in the room.
Liver Battery (Liver Function Studies)
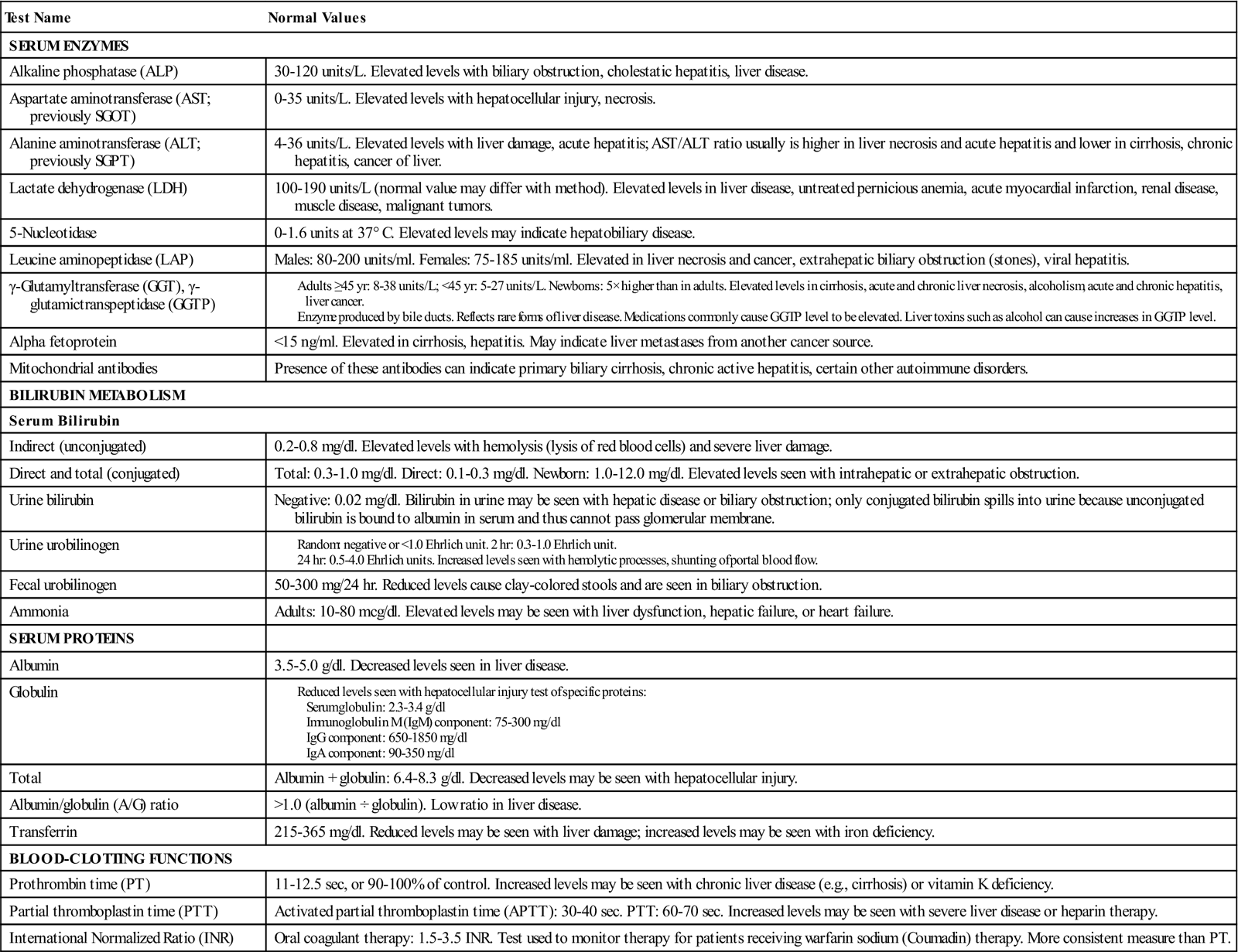
Modified from Liver disease: common liver function tests, 2005, available at www.umm.edu/liver/tests.htm. Accessed April 1, 2009; Pagana KD, Pagana TJ: Mosby’s diagnostic and laboratory test reference, St Louis, 2009, Mosby; Serum globulin electrophoresis, 2005, available at www.nlm.nih.gov/medlineplus/ency/article/003544.htm. Accessed April 1, 2009.
When anticipating an operative cholangiogram, the surgical technologist must ensure that the OR bed has been equipped and positioned so that C-arm image intensification can be accomplished efficiently. Radiation-protection devices for the surgical team and patient should be available.
Thermoregulation.
The risks of intraoperative hypothermia have been well documented. When laparotomy is performed, patients are at further risk for hypothermia. To prevent unplanned hypothermia, the surgical technologist takes affirmative measures to maintain body temperature in the OR (Insler and Sessler, 2006). The environmental temperature and humidity are set to prevent body heat loss caused by evaporation and convection. A forced-air warming blanket placed over the patient’s upper body, head, and neck assists in maintenance of body temperature. Minimizing body exposure to ambient air and the use of warm irrigating solutions also support thermoregulation. The temperature of irrigating fluids should be no higher than body temperature (37° C; 98.6° F) (AORN, 2009). A blood- and fluid-warming device may be used by the anesthesia provider to deliver intravenous (IV) fluids at a temperature higher than room air temperature. The anesthesia provider commonly monitors the patient’s core temperature by use of an esophageal temperature probe when the duration and complexity of the surgical procedure place the patient at risk for hypothermia. Additional comfort measures include using warm blankets before and after surgery.
Application of Sequential Compression Device.
Patients undergoing lengthy surgical procedures are at risk for venous dilation and blood pooling in the lower extremities. This may predispose the surgical patient to develop venous thromboembolism (VTE) in the postoperative period. Sequential compression devices (SCDs) are frequently applied in the OR before commencing lengthy surgical procedures in order to prevent or minimize VTE risks.
Draping the Patient.
After the abdominal prep, time must be allowed for the prep solution to dry and vapors to dissipate. This is an essential patient safety precaution when flammable prep solutions are used in conjunction with electrosurgery (or other ignition sources, such as a laser). Sterile towels are then arranged to accommodate the intended incision. A sterile drape sheet may be placed over the patient’s lower torso and a laparotomy sheet is then placed to provide a wide sterile field and to cover all exposed body surfaces except the incision site.
Instrumentation.
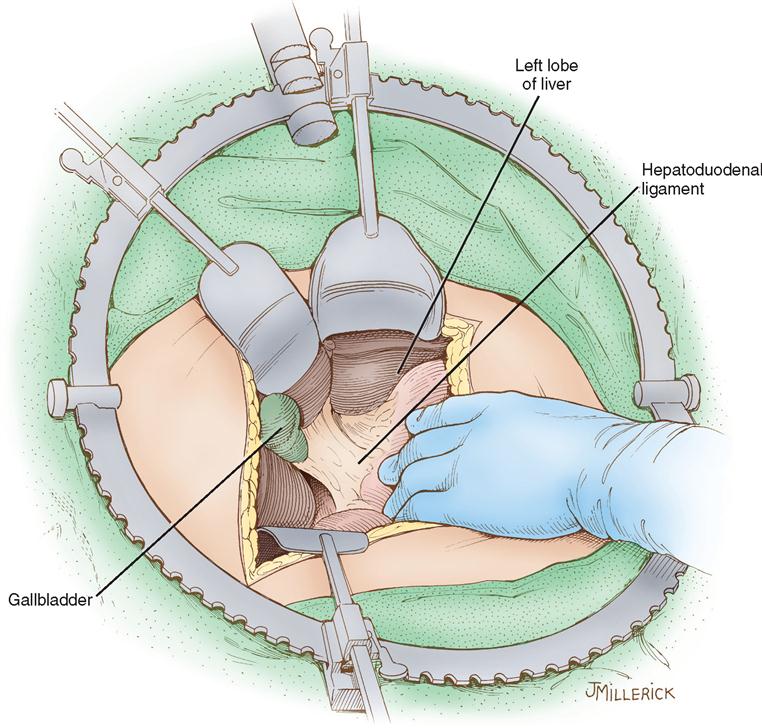
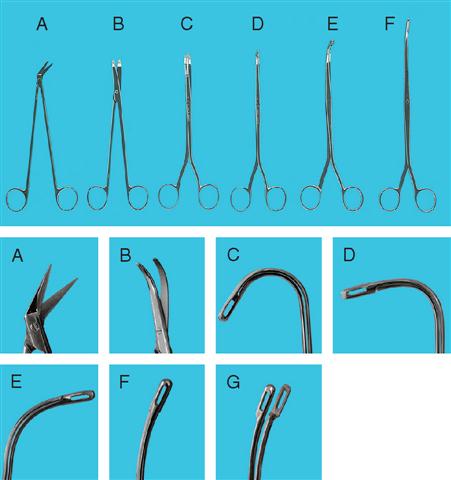
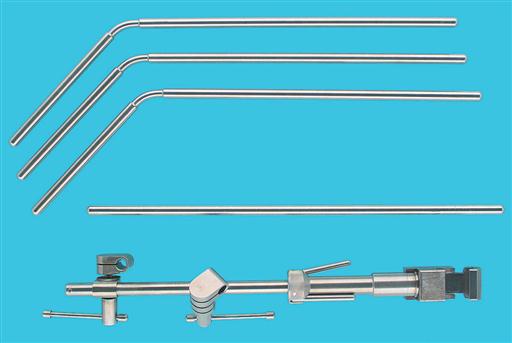
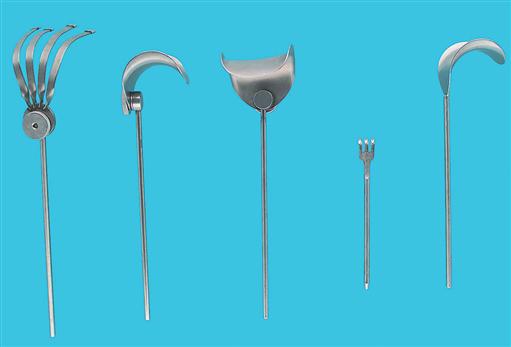
Instrumentation for open (i.e., performed via a laparotomy incision) surgeries of the liver, biliary tract, spleen, and pancreas includes a basic laparotomy set, biliary probes and forceps for dilating and exploring the ducts of the pancreas and biliary tract, vascular clamps, gastrointestinal (GI) clamps, and ligating clips and appliers of all sizes. Linear stapling instruments also should be available. A self-retaining system such as the Bookwalter retractor set (Figure 3-6) provides excellent exposure of the abdominal viscera. In addition, a flexible choledochoscope, Cavitron ultrasound suction aspirator (CUSA), intraoperative ultrasound, laser, argon beam coagulator, harmonic scalpel, and electrosurgical unit (ESU) may be required to perform certain procedures on the hepatobiliary system. Safe practices when using devices that generate surgical smoke require the use of a smoke evacuation system and accessories in both open and laparoscopic procedures (AORN, 2009). See Figures 3-7 through 3-14 for common instruments used in procedures of the liver, biliary tract, and spleen.
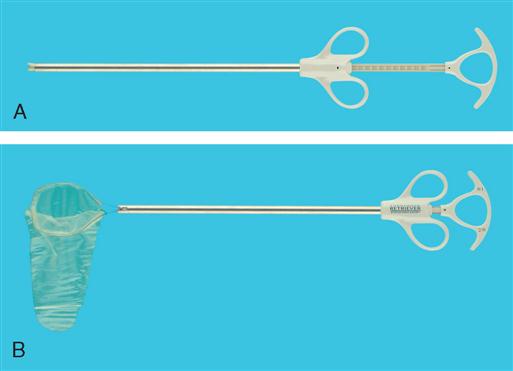




The basic equipment for minimally invasive surgical (MIS) procedures consists of two high-density monitors, an insufflation unit, ESU, light source, camera, and 0-degree and 30-degree telescopes in 10-mm and 5-mm sizes. A printer is optional. An ultrasonic dissecting unit is often used with MIS procedures. Trocars and sleeves are available in reusable, disposable, and resposable designs. Trocars and sleeves are commonly designed to accommodate 10-mm to 5-mm instruments and 12-mm to 5-mm accessories and instruments. MIS instruments include scissors and shears, dissecting forceps, atraumatic grasping forceps, hooks, Babcock clamps, retractors, needles, suturing devices, pouches, suction-irrigating devices, and mechanical stapling devices.
Thrombin, Gelfoam, Surgicel, Avitene, and other chemical hemostatic agents (Surgical Pharmacology) should be available in the OR suite. Radiographic dye, supplies, and radiation-protection devices will be required if intraoperative radiography or angiography is planned as part of the procedure.
Drainage Materials.
Tubes and catheters are selected for the areas to be drained. If a defective drain is used, a free fragment may remain in the wound on removal of the tube. Thus the surgical technologist should note the condition of all drainage materials and should test them for patency before they are placed in the patient.
Soft rubber or latex tissue drains may be used after an open cholecystectomy or a choledochostomy. Verify that the patient has no latex allergy before using these devices and substitute nonlatex drains if necessary (Risk Reduction Strategies). The surgeon will prepare a latex rubber T-tube drain of suitable size after exploring the duct. The center of the crossbar is notched opposite the junction of the vertical limb so that its ends will bend more readily during removal. The ends are beveled and tailored to fit the duct.
Drains are usually exteriorized through separate stab wounds and anchored to skin edges to prevent their retraction.
Aseptic Considerations.
When the common duct is opened or an anastomosis is established between a duct and other parts of the alimentary tract, it may be the institution’s policy or the surgeon’s preference to isolate contaminated instruments and materials from the remainder of the operative field, as described for GI surgery (Chapter 2). The wound is classified according to a standard system: any procedure in which the alimentary tract is entered under controlled conditions and without unusual contamination is considered a clean contaminated wound; if there is gross spillage, however, the wound is classified as contaminated. Proper wound classification is considered an important predictor of postoperative SSI (Phillips, 2007; Meakins and Masterson, 2007).
Chemical Hemostatic Agents
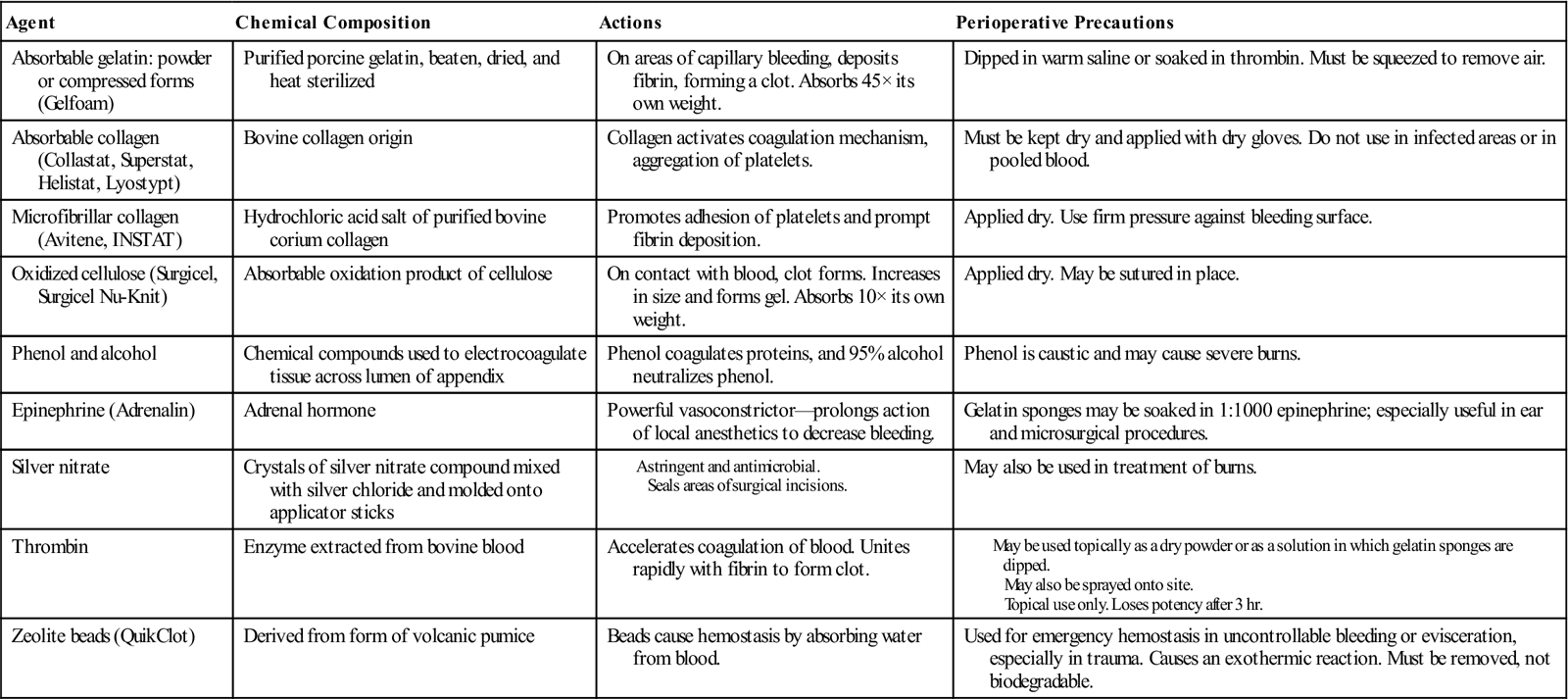
Modified from Phillips NF: Berry and Kohn’s operating room technique, ed 11, St Louis, 2007, Mosby.
Blood Products.
During the preoperative verification process, the surgical team should ascertain the type and amount of blood and blood products, both requested and available, as well as ensure the patient has a signed consent for transfusion. Constant, ongoing evaluation of blood loss is communicated to the anesthesia provider and surgical team during the procedure. When additional blood or blood products are required, the perioperative nurse communicates with blood bank personnel so that products are readily available and carries out the required steps to verify blood/blood products with the anesthesia provider before transfusion.
Autologous blood or donor-directed blood products may be used in elective procedures involving the liver, pancreas, spleen, and biliary tract. Cell-saver devices may be used when potential contamination of the blood from bile or bowel does not exist.
Latex Sensitivity and Allergy Guidelines
Natural rubber latex allergy can be a serious and life-threatening condition. Healthcare workers and others who have experienced repeated exposure to latex can develop latex sensitivity or allergy. The following is a list of guidelines that should be instituted in persons with suspected or known latex sensitivity or allergy:
♦ Identify the patient’s risk factors and report them to the OR team. Those at high risk include persons with the following:
• Multiple surgeries, particularly if begun in early infancy
• A positive serum latex antibody test
• Occupational exposure to latex products, particularly powdered products
• Allergy to bananas, kiwi, avocado, stone fruits, raw potato, tomato, papaya, chestnuts
♦ Notify the anesthesia department and OR 24 to 48 hours in advance.
♦ Notify healthcare providers in other perioperative areas of the patient’s latex sensitivity status.
♦ Plan for a latex-safe environment of care:
• Remove all latex products from the room unless no alternative exists.
• Obtain a latex-free cart from the designated area.
• Place a latex precaution card on the OR door.
Modified from Association of periOperative Registered Nurses (AORN): Perioperative standards and recommended practices, Denver, 2009, The Association; Brown RH et al: The final steps in converting a health care organization to a latex-safe environment, Jt Comm J Qual Patient Saf 35(4):224-228, 2009; Phillips N: Berry and Kohn’s operating room technique, ed 11, St Louis, 2007, Mosby.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


